
Robot assisted laparoscopic abdominal cerclage: two case reports
Authors:
R. Pilka; K. Huml; M. Lubušký; J. Vodička; V. Jančeková; V. Kolářová
Authors‘ workplace:
Department of Obstetrics and Gynecology, University Hospital Olomouc, Faculty of Medicine and Dentistry, Palacký University, Olomouc, head of department prof. MUDr. R. Pilka, Ph. D.
Published in:
Ceska Gynekol 2018; 83(3): 195-200
Overview
Objective:
In this work we report the first use of robot-assisted preconceptual abdominal cerclage in the Czech Republic with subsequent live birth. We present two patients with a history of late pregnancy losses (late miscarriage) who underwent robotic abdominal cerclage.
Design:
Case report.
Setting:
Department of Obstetrics and Gynecology, University Hospital Olomouc, Faculty of Medicine and Dentistry, Palacký Univesity, Olomouc.
Methods:
The da Vinci S surgical system was used for the robot-assisted abdominal cerclage.
Results:
One robot-assisted laparoscopic transabdominal cerclage patient delivered at term a live infant and the second patient currently undergoes infertility treatment with in vitro fertilization.
Conclusion:
Robotic abdominal cerclage is a relatively new minimally invasive method for treatment of cervical insufficiency. This technique provides 3D visualization and better instrumentation than the conventional laparoscopic approach.
Keywords:
robotic abdominal cerclage, laparoscopy, cervical insufficiency
INTRODUCTION
One of the leading causes of perinatal infant morbidity and mortality is cervical insufficiency [1]. It occurs in 0,5%–1% of all pregnancies and has a recurrence risk of up to 30% [5, 21]. In 1955, Shirodkar proposed a transvaginal cerclage for the treatment of cervical insufficiency [22]. McDonald later simplified the procedure in 1957, and the McDonald technique is now the most commonly used [17]. Transabdominal cerclage was introduced in 1965 by Benson and Durfee, as a procedure reserved for patients with either a poor obstetric history, patients who experience a failed prophylactic transvaginal cerclage or in whom a transvaginal cerclage is not technically possible [3]. With the introduction of the transabdominal cerclage, the fetal survival rate improved from 21 to 89% [20]. Despite the significantly improved fetal outcomes, subsequent studies suggested increased surgical morbidity for women undergoing transabdominal cerclage via laparotomy as compared to transvaginal cerclage [14]. Laparoscopic transabdominal cerclage is associated with faster recovery, fewer adhesions, less postoperative pain and less hospitalisation than an open approach and it has comparable rates of third trimester delivery and live birth [16]. Due to technical difficulties and limitations of the laparoscopic surgery, laparoscopic abdominal cerclage has not gained widespread popularity [9, 13]. Robotic-assisted laparoscopic transabdominal cerclage surgery is an emerging technology with promising possibilities and practical implications [2]. The robotic cerclage is an alternative to an open procedure with all the above mentioned benefits of laparoscopy. The improved visualisation and articulated dissection with robotics, along with the potential for reduced venous bleeding represents a potential for more patients to benefit from this surgery [6, 18, 19]. In this report we present the first use of robot-assisted preconceptual abdominal cerclage in the Czech Republic with subsequent live birth.
CASE REPORTS
We present two patients with a history of late pregnancy losses (late miscarriage) who underwent robotic (one case) abdominal cerclage and subsequently achieved pregnancy. The da Vinci S surgical system was used for the robot-assisted abdominal cerclage. One robot-assisted cerclage patient delivered a live infant and the second patient undergoes infertility programme with in vitro fertilization at this time.
The first case
A 38-year-old patient, gravida 4, para 2, with a history of one term delivery by vacuumextraction, one preterm delivery at 23 weeks’ gestation and one spontaneous abortion at 21 weeks’ gestation was preconceptually offered a robot-assisted abdominal cerclage by the da Vinci S surgical system. Following induction of general endotracheal anesthesia, 4 robotic port sites were placed as follows: (1) 12mm trocar in the midline above the umbilics for the camera, (2) 8mm robotic trocar on the right side 2 cm above and medial to the right superior iliac crest for the monopolar scissors, (3) 8mm robotic trocar on the left side 2 cm above and medial to the left superior iliac crest for the atraumatic forceps, (4) 8mm robotic trocar 8 cm to the left to the camera port for the Maryland bipolar forceps. A 12-mm accessory port was also placed on the right upper quadrant for use of the suction irrigator and passage of the Mersilene tape. At the beginning preparation of the vesicouterine excavation and opening of the anterior leaf of the broad ligament were carried out. At the level of the uterine isthmus, along the edge of the uterus, the uterine arteries were released and preparation of “avascular windows” between the uterine artery and the appropriate uterine edge were carried out. After removal of the insertion needles a 30 cm long Mercilon tape was inserted into the abdominal cavity. Both tips of the tape were passed through the avascular windows and a knot was tied in front of the anterior uterine wall. The both free ends of the tape were finally fixed together via a hemolock clip (Figure 1). The procedure took 146 minutes and estimated blood loss was 50 ml. There was no intraoperative complication and the patient was discharged from hospital at the postoperative first day. Four months after the procedure the patient spontaneously conceived. She was followed up by the maternal fetal medicine and had an otherwise uncomplicated antepartum course. Images of the transvaginal ultrasound examination four months after the robotic procedure and at 25 weeks’ gestation are shown in Figure 2 and 3, respectively. Ultrasound verified correct placement of the cerclage (Figure 2) and a cervical length of 2.6 cm (Figure 3). She delivered a healthy female infant at 38 weeks via cesarean section. The cerclage was left in situ at the time of cesarean section.



The second case
A 37-year-old patient, gravida 3, para 1, with a history of two spontaneous abortions during the second trimesters and one preterm delivery at 35 weeks’ gestation was indicated to the preconceptual robot-assisted abdominal cerclage. The patient was offered to be operated with robotic surgery, for abdominal cerclage. After her acceptance, she underwent robotic surgery and the procedure was successfully completed in 51 minutes and estimated blood loss was 20 ml. The same surgical technique was used as in the first case. No surgical complications occurred during the intervention and the postoperative stay and no conversion to laparotomy. The patient was discharged from hospital one day after operation. Now she is attending an in vitro fertilization programme.
DISCUSSION
Increased neonatal survival rates are associated with transabdominal cerclage [8]. Historically, the transabdominal cerclage has required two open procedures – an open laparotomy to place the cerclage and a cesarean section at the time of delivery. Open laparotomies require an inpatient hospital stay and the increased risk of a number of morbidities: fever, adhesion formation, blood loss, ileus, venous thrombosis, and prolonged reduced aktivity [4]. Laparoscopic transabdominal cerclage represents an effective, minimally invasive alternative for patients in whom transvaginal cerclage is not possible. A few obstetrician-gynecologists have performed laparoscopic abdominal cerclages to reduce these morbidities. Complications of conventional laparoscopic cervical cerclage including bleeding, suture displacement, and failure of placement can often result from poor visualization and lack of manual dexterity [6]. Robot assisted laparoscopic abdominal cerclage has emerged as a viable alternative to the traditional open approach or laparoscopic approach [7, 11, 24, 25]. Robotic technology likely offers the benefits of increased precision in dissection and tying as compared to conventional laparoscopic approaches and decreased surgical morbidity as compared to laparotomy [19]. Abdominal cerclages are either placed before conception (interval cerclage) or during pregnancy in the late first or early second trimester. The first robot-assisted laparoscopic cerclage in a non-pregnant patient was performed by Barmat et al. in 2007 [2]. Fechner et al. reported in 2009 a case which included the first robotic assisted abdominal cerclage in a pregnant woman [6]. Subsequent studies concluded that although laparoscopy is now regarded as an acceptable approach to placement of transabdominal cerclage, robotic placement is a possible option for those in which simple laparoscopy may prove to be too difficult [7, 24–26] (table 1).
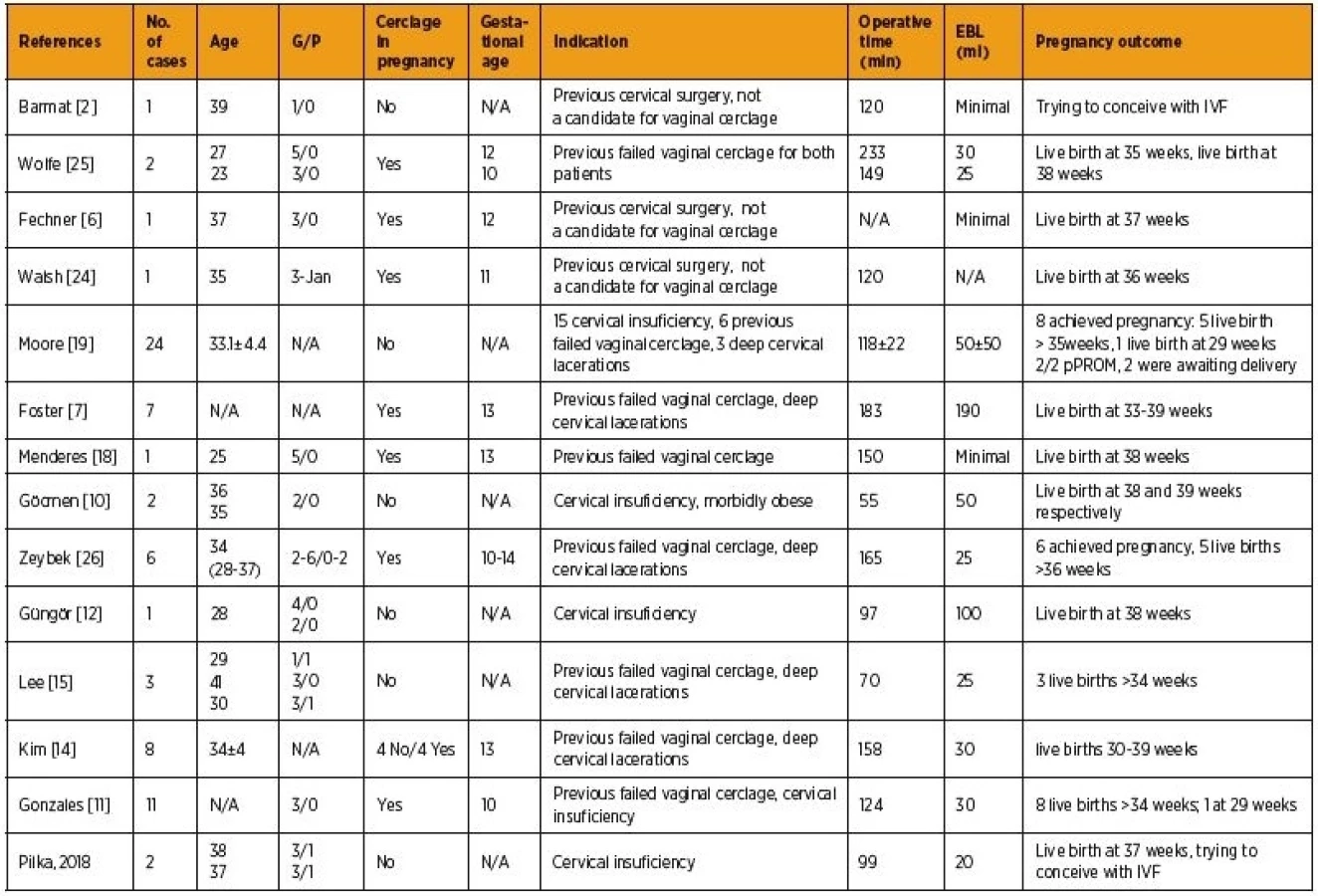
The most comprehensive study including robot-assisted abdominal cerclage was reported by Moore et al., in which a total of 24 nonpregnant patients underwent robotic procedure [19]. Only in one case a conversion to laparotomy due to dense adhesions has to be carried out. The mean operative and console times were reported to be 118 and 58 minutes, respectively.
The mean length of hospital stay was less than one day. Furthermore they compared the robotic surgical outcomes with conventional laparoscopy and stated that although the robotic procedure takes additional time to complete and requires longer exposure to anesthesia (155 minutes versus 103 minutes), it significantly shortens recovery time (21 hours versus 50 hours), decreases blood loss (50mL versus 150mL) and reveals to be less invasive [10].
In 2013, Foster et al. recruited seven patients for robotic cerclage placement. Six successfully completed their pregnancy and there was one fetal loss. Peroperative complication rate was low, but in one patient the blood loss exceeded 500 ml. A consistent problem was encountered with access to the upper cervix beyond the extremely soft, enlarged uterus. The procedure was converted to laparotomy in two cases with conclusion: robotic-assisted transabdominal cervical cerclage is an advantageous procedure in the non-pregnant individual, but should be approached cautiously during pregnancy [7].
Kim et al. published comparison of surgical and obstetric outcomes in 20 patients after transabdominal cerclage placed either by minimally invasive or open approach [14]. Of these, eight cerclages were performed using the daVinci robotic system. Authors revealed no statistically significant differences in obstetric outcomes between the laparotomy and laparoscopy groups. Among women who delivered after minimally invasive abdominal cerclage (n = 8), six (75%) delivered at 34 weeks or more. The rate of women accomplishing at least 34 weeks of gestation was 78% for the laparotomy group patients. In agreement with Tulandi, they found no difference in the rates of third trimester delivery and live birth between abdominal cerclage placed as an interval or post-conception procedure [14, 23].
In their series, Gonzales et al. report nine out of 11 (81.8%) primary robot assisted laparoscopic abdominal cerclage placement procedures resulted in a viable live-born neonate; eight (72.7%) were born >34 weeks of gestation [11].
Recently, Güngör et al. described successfully achieved robot assisted abdominal cerclage in morbidly obese patient (BMI > 35) with no peroperative complications, minimal blood loss and console time 61 min [12].
The main disadvantage of robotic procedures published in the literature is cost. Lee et al. have published case series comparing three cases of robotically placed cerclages, and two cases performed by laparotomy. All procedures were performed prior to pregnancy. The operating time was 53–102 min in robotic cases, and 66–83 min in laparotomy cases. They have shown that costs can be comparable when performing robot assisted and open transabdominal cerclages [15]. The higher cost in open transabdominal cerclage is related to two issues. First, the increased patient length of stay involved with the laparotomy procedure considerably increases the cost to the patient. Second, the cost of the roboticallyassisted procedure is based on the efficient use of the daVinci Surgical System at the institution one considers. A larger number of procedures with less downtime appreciably lowers the cost of using the equipment [19].
Herein we report the first two robot assisted transabdominal cerclages performed in a non-pregnant women in the czech literature, with subsequent pregnancy terminated by caesarean section at term in one of them.
CONCLUSION
The da Vinci robot-assisted surgical approach offers a minimally invasive alternative to exploratory laparotomy for the placement of transabdominal cerclage. Compared with conventional laparoscopy, the da Vinci facilitates transabdominal cerclage because of wristed instrumentation, high definition (HD) three-dimensional (3D) optics and autonomy of camera control. Further randomized and controlled trial studies are warranted to determine if robotic surgery truly offers a benefit over laparoscopy in terms of surgical outcomes.
This work was supported by the Palacky University via an institutional grant project IGA_LF_2018_001.
Corresponding author
Veronika Kolářová, MD
Department of Obstetrics and Gynecology
University Hospital Olomouc
Faculty of Medicine and Dentistry
Palacký University
I. P. Pavlova 6
775 20 Olomouc
e-mail: veronika.kolarova@fnol.cz
Sources
1. Al-Fadhli, R.,Tulandi, T. Laparoscopic abdominal cerclage. Obstet Gynecol Clin North Am, 2004, 31(3), p. 497–504, viii.
2. Barmat, L., Glaser, G., Davis, G., et al. Da Vinci-assisted abdominal cerclage. Fertil Steril, 2007, 88(5), p. 1437 e1–3.
3. Benson, RC., Durfee, RB. Transabdominal cervico uterine cerclage during pregnancy for the treatment of cervical incompetency. Obstet Gynecol 1965, 25, p. 145–155.
4. Dharia, SP., Falcone, T. Robotics in reproductive medicine. Fertil Steril, 2005, 84(1), p. 1–11.
5. Drakeley, AJ., Roberts, D., Alfirevic, Z. Cervical stitch (cerclage) for preventing pregnancy loss in women. Cochrane Database Syst Rev 2003(1):CD003253.
6. Fechner, AJ., Alvarez, M., Smith, DH., et al. Robotic-assisted laparoscopic cerclage in a pregnant patient. Am J Obstet Gynecol, 2009, 200(2), p. e10–1.
7. Foster, TL., Addleman, RN., Moore, ES., et al. Robotic-assisted prophylactic transabdominal cervical cerclage in singleton pregnancies. J Obstet Gynaecol, 2013, 33(8), p. 821–822.
8. Foster, TL., Moore, ES., Sumners, JE. Operative complications and fetal morbidity encountered in 300 prophylactic transabdominal cervical cerclage procedures by one obstetric surgeon. J Obstet Gynaecol, 2011, 31(8), p. 713–717.
9. Ghomi, A., Rodgers, B. Laparoscopic abdominal cerclage during pregnancy: A case report and a review of the described operative techniques. J Minim Invasive Gynecol 2006, 13(4), p. 337–341.
10. Gocmen, A., Sanlikan, F. Two live births following robotic-assisted abdominal cerclage in nonpregnant women. Case Rep Obstet Gynecol, 2013, 2013, p. 256972.
11. Gonzales, SK., Adair, CD., Torres, C., et al. Robotic-assisted laparoscopic abdominal cerclage placement during pregnancy. J Minim Invasive Gynecol, 2017.
12. Gungor, M., Afsar, S., Ozbasli, E., et al. The interval robotic transabdominal cerclage in a morbidly obese patient. J Robot Surg, 2016, 10(1), p. 69–72.
13. Huml, K., Kantor, L., Prochazka, M., et al. [Laparoscopic abdominal cerclage in a patient with recurrent miscarriages abortions – case report]. Ces Gynek, 2016, 81(1), p. 58–62.
14. Kim, S., Hill, A., Menderes, G., et al. Minimally invasive abdominal cerclage compared to laparotomy: a comparison of surgical and obstetric outcomes. J Robot Surg, 2017.
15. Lee, R., Biats, D., Mancuso, M. Robotic transabdominal cerclage: a case series illustrating costs. J Robot Surg, 2017.
16. Luo, L., Chen, SQ., Jiang, HY., et al. Successful treatment of cervical incompetence using a modified laparoscopic cervical cerclage technique: a cohort study. Eur J Obstet Gynecol Reprod Biol, 2014, 179, p. 125–129.
17. McDonald, IA. Suture of the cervix for inevitable miscarriage. J Obstet Gynaecol Br Emp, 1957, 64(3), p. 346–350.
18. Menderes, G., Clark, L., Azodi, M. Robotic-assisted abdominal cerclage: a case report and literature review. J Robot Surg, 2014, 8(3), p. 195–200.
19. Moore, ES., Foster, TL., McHugh, K., et al. Robotic-assisted transabdominal cerclage (RoboTAC) in the non-pregnant patient. J Obstet Gynaecol, 2012, 32(7), p. 643–647.
20. Novy, MJ. Transabdominal cervicoisthmic cerclage: a reappraisal 25 years after its introduction. Am J Obstet Gynecol, 1991, 164(6 Pt 1), p. 1635–1641, discussion 1641–1642.
21. Shennan, A., Jones, B. The cervix and prematurity: aetiology, prediction and prevention. Semin Fetal Neonatal Med, 2004, 9(6), p. 471–479.
22. Shirodkar, VN. Tendences acutelles en Gynécologie et Obstétriques. Geneva: Librairie de l´Université, 1955.
23. Tulandi, T., Alghanaim, N., Hakeem, G., et al. Pre and post-conceptional abdominal cerclage by laparoscopy or laparotomy. J Minim Invasive Gynecol, 2014, 21(6), p. 987–993.
24. Walsh, TM., Borahay, MA., Fox, KA., et al. Robotic-assisted, ultrasound-guided abdominal cerclage during pregnancy: overcoming minimally invasive surgery limitations? J Minim Invasive Gynecol, 2013, 20(3), p. 398–400.
25. Wolfe, L., DePasquale, S., Adair, CD., et al. Robotic-assisted laparoscopic placement of transabdominal cerclage during pregnancy. Am J Perinatol, 2008, 25(10), p. 653–655.
26. Zeybek, B., Hill, A., Menderes, G., et al. Robot-assisted abdominal cerclage during pregnancy. JSLS, 2016, 20(4).
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology

2018 Issue 3
Most read in this issue
- Prolactin and alteration of fertility
- Does EmbryoGlue transfer medium affect embryo transfer success rate?
- Vaccination against HPV and view of new possibilities
- Planned home births in the Czech Republic, 2018