
Epidemiological characteristics of human leptospirosis in Slovak Republic, 2008–2019
Authors:
J. Perželová; M. Kotrbancová; M. Fulová; A. Bražinová
Authors‘ workplace:
Comenius University in Bratislava, Faculty of Medicine, Institute of Epidemiology, Bratislava, Slovak Republic
Published in:
Epidemiol. Mikrobiol. Imunol. 74, 2025, č. 3, s. 141-148
Category:
Original Papers
doi:
https://doi.org/10.61568/emi/11-6568/20250808/141313
Overview
Aim of study: The purpose of this study was observation of some epidemiological characteristics of human leptospirosis in Slovakia during 2008–2019.
Materials and Methods: Patients’ data analysed in this work were obtained from laboratory diagnostic and trawling questionnaires. The diagnosis of acute leptospirosis was confirmed by the serological examination in the micro-agglutination test in accordance with clinical and epidemiological data. Statistical analyses were performed by software STATA version 18 (StataCorp LP, College Station, TX, USA).
Results: Average annual incidence rate in Slovakia in the study period was 0.185/100,000 population. Case-fatality rate was 2.48% due to three fatal cases. The infection affected more men (80.16%) than women (19.84%) mostly in the age of 20–69 years old with the peak in 50–59 years old. Almost three quarters of affected persons were people without professional exposure. The highest number of cases was recorded in the period from June to November, peaking in August (25.62%). The most cases of infections were reported from administrative regions Košice (23.14%) and Trenčín (22.31%).
Conclusions: Incidence rate of human leptospirosis maintains the declining character in the study period, which has been present in recent decades in Slovakia. The numbers are most likely underreported, due to the misdiagnosing of leptospirosis cases caused by broad spectrum of clinical manifestations and low awareness of clinicians of possible diseases etiology.
Keywords:
Epidemiology – Leptospira – human diseases – incidence rate
INTRODUCTION
Leptospirosis is worldwide occurring zoonosis caused by pathogenic bacteria of the genus Leptospi ra [20, 25, 26, 27]. Human infection occurs after direct contact with an infected animal reservoir, but more often is transmitted indirectly, through the water and moist soil contaminated by the urine of infected animals. The most important reservoirs are rodents, small mammals, cattle, pigs, sheep and horses [26].
The usual portal of entry are abrasions or cuts in the skin, the mucous membranes of the oral and nasal cavities or conjunctiva. Human leptospirosis ranges in its clinical spectrum from mild to lethal courses. It may not have any clinical manifestation, or it may manifest as a febrile influenzalike disease, meningoencephalitis, in the form of pulmonary haemorrhages with respiratory failure or as fatal hepato-renal syndrome [28]. Incidence of human leptospirosis is affected by environmental and socioeconomic factors, which differ among countries and change over time. The incidence rate in developed countries with temperate climate is between 0.1–1/100,000 population and in tropical and subtropical countries it is reported to be more than 10/100,000 [1]. A disease incidence rate rises when seasonal outbreaks occur or within the risk groups with professional or social exposure [1]. Absent or inadequate notification system in some countries contributes to underestimated global incidence rate of human leptospirosis [18], which is 1 million cases annually with almost 60,000 deaths worldwide [16]. Another significant factor of underreporting is misdiagnosing of leptospirosis due to broad spectrum of nonspecific clinical characteristics or not recognizing the mild cases of disease [18]. Although leptospirosis is more significant public health problem in developing and humid tropical countries than in temperate climate [25, 27], in the past, leptospirosis was historically important human disease in Slovakia with incidence rate up to 5/100,000 and epidemic occurrence. It has been studied in Slovakia since 1949, when the laboratory diagnosis of leptospirosis was introduced and systematic surveillance is carried out since 1970 [12]. Notification of leptospirosis is mandatory in Slovakia and laboratory diagnosis is performed in one workplace for the whole country, in Bratislava, the capital city localized in Western Slovakia. The objective of this study is to describe current trends in epidemiology of human leptospirosis in Slovakia, with a focus on reported acute cases in the period from 2008 to 2019. The findings may contribute to investigation and knowledge of the burden of this disease and so may be useful for programs aimed at its prevention and control.
MATERIALS AND METHODS
This study summarizes epidemiological characteristics of human leptospirosis in Slovakia in past twelve years (2008–2019). All reported cases of leptospirosis were diagnosed at the Institute of Epidemiology, Faculty of Medicine, Comenius University in Bratislava, which is the only national diagnostic laboratory for human leptospirosis in the country. All 121 patients´ data analysed in this work were obtained from laboratory diagnostic and trawling questionnaires [2, 3, 4, 5, 6, 7, 8, 9, 10, 11].
Variables evaluated in this study were the following: incidence rate, etiology, distribution of cases in selected professional categories and social groups, age-specific and gender-specific rates, seasonality, geographical distribution and clinical forms of the disease. The diagnosis of acute leptospirosis of all 121 patients was confirmed by the serological examination of sera samples in the microagglutination test by a 4-fold increase in antibody titre or, in the case of a single serum sample, by a titre ≥ 1 : 1,600 in accordance with clinical and epidemiological data. The set of Leptospira strains was used and encompassed pathogenic and saprophytic strains representing serological groups Icterohaemorrhagiae, Grippotyphosa, Sejroe, Javanica, Pomona, Canicola, Australis, Tarassovi, Bataviae, Ballum, Autumnalis, Pyrogenes, Andamana and Semaranga. Leptospiral strains were cultivated 10–14 days at 29 °C in liquid Korthof’s medium enriched with yeast extract and rabbit serum. All statistical analyses were performed by software STATA version 18 (StataCorp LP, College Station, TX, USA).
RESULTS
During the period of 2008–2019, 121 patients with acute leptospirosis were diagnosed and reported in Slovakia. Out of the total number of analysed samples, 1.9% were positive in this period. Total incidence rate of human leptospirosis ranges from 0.42/100,000 to 0.04/100,000 population. Average annual incidence rate was 0.185/100,000 [2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. In
Figure 1 we present incidence rate of leptospiral infections in Slovakia since 1949 till 2019. Incidence rate for the period 2008–2019 is displayed in Table 1, together with 95% confidence interval. During the study period, three fatal cases were reported in 2009, 2010 and 2015, case-fatality rate was 2.48%.
Most of the cases (53.72%) were classified as Weil’s disease caused by serovars Icterohaemorrhagiae and Copenhageni (33.89%) followed by leptospirosis caused by serovar Grippotyphosa (19.83%). Unexpectedly high proportion (12.4%) of etiologically unsolved patients (in the group “other”) was recorded, including those, whose sera showed paradoxical reactions typical for an early stage of acute leptospirosis. The rest of infections were caused by serovars Australis (12.4%), Sejroe (10.74%) and Pomona (10.74%). Fatal cases of leptospirosis were caused by serovars Icterohaemorrhagiae+Copenhageni, Australis and one fatal infection was reported as paradoxical reaction (Table 2).
A total of 97 male patients (80.16%) and 24 female patients (19.84%) with leptospirosis were reported in 2008–2019, of which two females and one male have died. In both males and females, the main infecting serovars were Icterohaemorrhagiae + Copenhageni. In men, these serovars caused 28.1% of infections and in women 5.79% (see Table 2).

Table 1. Annual incidence rate of human leptospirosis in Slovakia, 2008–2019
|
Year |
Incidence rate per 100,000; 95% CI [LL, UL] |
Number of positive patients |
Number of positive samples/number of analysed samples* |
|
2008 |
0.31; [0.2, 0.51] |
17 |
32/1562 |
|
2009 |
0.37; [0.24, 0.57] |
20 |
38/1890 |
|
2010 |
0.42; [0.28, 0.64] |
23 |
44/2098 |
|
2011 |
0.15; [0.07, 0.3] |
8 |
30/1757 |
|
2012 |
0.17; [0.09, 0.32] |
9 |
21/1214 |
|
2013 |
0.07; [0.03, 0.2] |
4 |
11/1119 |
|
2014 |
0.22; [0.13, 0.39] |
12 |
20/1235 |
|
2015 |
0.17; [0.09, 0.32] |
9 |
20/954 |
|
2016 |
0.18; [0.1, 0.34] |
10 |
23/870 |
|
2017 |
0.07; [0.03, 0.2] |
4 |
13/722 |
|
2018 |
0.04; [0.01, 0.15] |
2 |
17/757 |
|
2019 |
0.05; [0.02, 0.17] |
3 |
13/696 |
Explanations:
CI – confidence interval; LL – lower level; UL – upper level; *some patients had several samples analysed
Table 2. Human leptospirosis by etiologic serovars in males and females in Slovakia, 2008–2019
|
Serovar |
Males n [%] |
Females n [%] |
Total n [%] |
|
IC + CO |
34 [28.1] |
7 [5.79] |
41 [33.89] |
|
GTY |
19 [15.7] |
5 [4.13] |
24 [19.83] |
|
SEJ |
11 [9.09] |
2 [1.65] |
13 [10.74] |
|
POM |
10 [8.26] |
3 [2.48] |
13 [10.74] |
|
AUS |
12 [9.92] |
3 [2.48] |
15 [12.4] |
|
Other |
11 [9.09] |
4 [3.31] |
15 [12.4] |
|
Total n [%] |
97 [80.16] |
24 [19.84] |
121 [100] |
Explanations:
IC + CO – Icterohaemorrhagiae + Copenhageni; GTY – Grippotyphosa; SEJ – Sejroe; POM – Pomona; AUS – Australis
During our study period, almost three quarters (74.38%) of affected persons were people without professional exposure to leptospires, for example administrative worker, lawyer, postman, ambulance driver and people without occupation, such as pupils, students, pensioners, housewives and unemployed people. Unemployed people and people with no-risk occupations in terms of exposure to leptospires are included in the group “other”. On the contrary, people with professional exposure, such as farmers, workers, slaughterhouse workers and field workers accounted only for 25.62% (Table 3).
Most of human leptospirosis cases (22.31%) as well as the highest incidence rate (0.298/100,000) were reported in the 50–59 years old age group, followed by 60–69 and 20–49 years old age groups. During the whole study period no infections were reported in children under 10 years old (Figure 2).
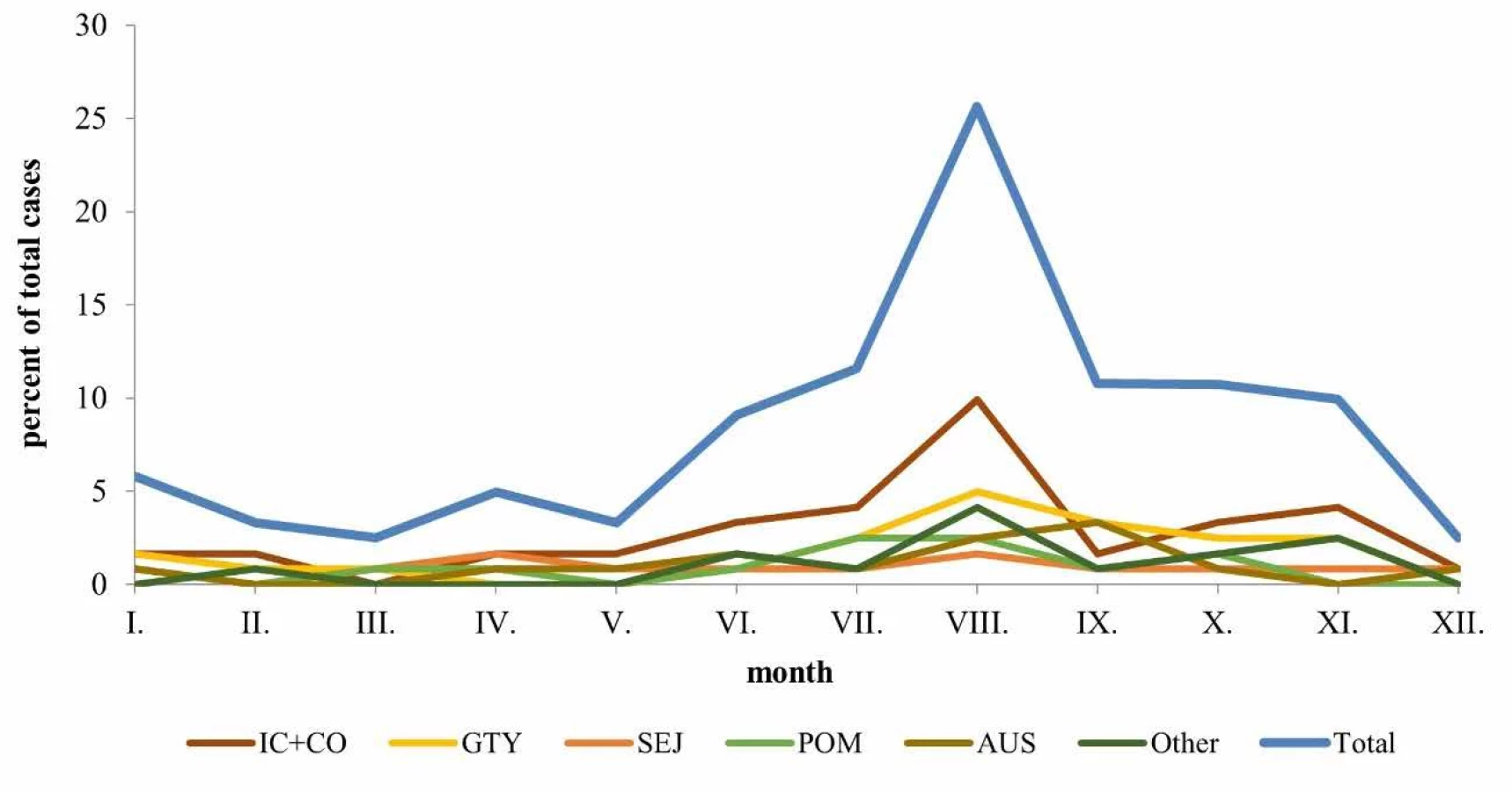
Further we have looked at seasonal occurrence. The highest number of cases in Slovakia was recorded in August (25.62%), mainly due to the incidence of leptospiroses caused by serovars Icterohaemorrhagiae + Copenhageni (9.92%) and Grippotyphosa (4.96%). Leptospiral infections caused by other serovars occurred uniformly, without peaks throughout the year. One fatal infection started in November and two in August (Figure 3).
Out of 121 patients, 18.21% had severe course of infection, 59.47% of patients had moderate course and 19.01% had mild course of the disease. In 3.31% of cases the course of the disease and symptoms were not documented. The course of the disease was evaluated according to the severity of the symptoms, complications and a need and length of hospitalization. Mild diseases were characterized as mild febrile illness, while severe diseases were characterized as renal disorders, hepatosplenomegaly, hemorrhagic manifestations or severe lung damage. Icteric forms are typical for Weil’s disease with present symptoms like yellow sclerae, dark urine and light stool. In febrile forms, the most significant symptom is fever associated with weakness, lassitude, chills and shivering. Meningeal forms are accompanied by positive meningeal signs, aseptic meningitis or meningoencephalitis. Icteric form was present in 30.59% of cases, febrile in 45.45%, meningeal form in 18.16%, the form of 3.31% cases was not documented and 2.49% of cases had other forms of infection – a nodal form, a hemorrhagic form and hepato-renal syndrome (Figure 4).
Table 3. Proportion of human leptospirosis by occupation in Slovakia, 2008–2019
|
Occupation/serovar n [%] |
IC+CO |
GTY |
SEJ |
POM |
AUS |
Other |
Total n [%] |
|
Farmers |
5 [4.13] |
0 [0] |
0 [0] |
2 [1.64] |
0 [0] |
0 [0] |
7 [5.77] |
|
Workers |
5 [4.13] |
3 [2.48] |
1 [0.83] |
0 [0] |
2 [1.64] |
2 [1.64] |
13 [10.72] |
|
Slaughterhouse workers |
0 [0] |
0 [0] |
1 [0.83] |
1 [0.83] |
0 [0] |
0 [0] |
2 [1.66] |
|
Field workers |
3 [2.48] |
2 [1.64] |
2 [1.65] |
1 [0.83] |
1 [0.83] |
0 [0] |
9 [7.43] |
|
Pupils, students |
5 [4.13] |
4 [3.3] |
1 [0.83] |
0 [0] |
0 [0] |
1 [0.83] |
11 [9.09] |
|
Pensioners, housewives |
10 [8.28] |
5 [4.13] |
4 [3.3] |
3 [2.48] |
7 [5.8] |
4 [3.3] |
33 [27.29] |
|
Other |
13 [10.74] |
10 [8.28] |
4 [3.3] |
6 [4.96] |
5 [4.13] |
8 [6.63] |
46 [38.04] |
|
Total n [%] |
41 [33.89] |
24 [19.83] |
13 [10.74] |
13 [10.74] |
15 [12.4] |
15 [12.4] |
121 [100] |
Explanations:
IC + CO – Icterohaemorrhagiae + Copenhageni; GTY – Grippotyphosa; SEJ – Sejroe; POM – Pomona; AUS – Australis

Three patients diagnosed during our study period died of severe course of the disease. All of them had icteric form of leptospirosis. The first one was 41 years old woman from Levice district (administrative region Nitra) with Weil‘s disease (caused by serovars Icterohaemorrhagiae + Copenhageni). She was unemployed, living in low hygienic standard and she worked in damp soil after the flood. She died due to acute hepato-renal failure shortly after hospitalization. The second case was 33 years old man with leptospirosis caused by serovar Australis from Žilina district (administrative region Žilina). He was unemployed, alcoholic, he had liver cirrhosis and died during re-hospitalization. The third patient was 30 years old, unemployed woman with paradoxical reaction. She lived in Bytča district (administrative region Žilina) in low hygienic standard, in wooden hut without water supply. She had liver cirrhosis and died shortly after re-hospitalization due to hemorrhagic shock.
IC + CO – Icterohaemorrhagiae + Copenhageni; GTY – Grippotyphosa; SEJ – Sejroe; POM – Pomona; AUS – Australis

IC + CO – Icterohaemorrhagiae + Copenhageni; GTY – Grippotyphosa; SEJ – Sejroe; POM – Pomona; AUS – Australis
Slovakia is divided into 8 administrative regions. Most of the infections in the study period were reported from Košice region (23.14%), which is located in Eastern Slovakia and Trenčín region (22.31%) in Western Slovakia. The lowest number of infections was reported from Banská Bystrica region (3.31%) in Central Slovakia and Bratislava region (4.13%) located in Western Slovakia (Figure 5).

BA Bratislava; TT Trnava; NR Nitra; TR Trenčín; BB Banská Bystrica; ZA Žilina; PO Prešov; KE Košice
DISCUSSION
In our study we have described incidence of human leptospirosis in Slovakia. An average annual incidence rate of human leptospirosis during the period of 2008–2019 in Slovakia was 0.185/100,000 population. Higher incidence rate (0.42/100,000 and 0.37/100,000 population) in 2010 and 2009 may be related to weather conditions such as high temperature and humidity. These conditions allow leptospires to survive outside of the host organism, but they are also suitable for the reproduction and survival of host organisms (especially rodents and small mammals). Temperatures during the year 2009 were average, but the months of April, July, August and November were unusually warmer. Higher numbers of diseases have also been reported in these months (55%). Precipitation was above normal in the seven months of this year. The year 2010 was warmer than previous years with regular and heavy precipitation. The summer months were high above average in terms of temperature and precipitation, and floods occurred. This was reflected in the number of diseases (87%) in the summer and autumn months [10].
The value of 0.185/100,000 represents more than tenfold decrease in comparison to period 1954 to 1963 when the average annual incidence rate was 2.08/100,000 [12]. Low occurrence of human leptospirosis cases was documented also in other developed countries including neighboring countries. Austria and the Czech Republic reported average incidence rate 0.2/100,000 population, Hungary 0.1/100,000 population and Poland 0.01/100,000 population in the years 2010–2019 [14]. The absence of outbreaks and changes in social and economic life of Slovak population over time, such as mechanization of industry, reduction of agricultural workers, improvement of personal protection or better opportunities for housing and food storage conditions may contribute to the decreasing trend in notified incidence rate in Slovakia [12]. However, the incidence rate is most likely underreported due to the misdiagnosing of leptospirosis cases caused by broad spectrum of clinical manifestations and low awareness of clinicians of possible etiology of diseases, when patients respond well to the treatment. This is reflected in decreasing number of samples annually sent for examination.
In the study period an increase in number of leptospirosis cases caused by serovars Icterohaemorrhagiae and Copenhageni, Australis and paradoxical reactions occurred, but fewer serovars were involved in human infections than in the past [12, 13]. Currently, most infections are caused by serovars Icterohaemorrhagiae and Copenhageni (33.89%) and Grippotyphosa (19.83%) [2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. In the past, majority of cases were caused by serovars Sejroe and Grippotyphosa [12, 13]. Some leptospira serovars are selectively bound to certain animal species. Therefore, the spectrum of causative serovars depends on which animal the affected person has been in contact with or on the particular environment. For the Sejroe serovar, the main host is the Mus musculus and the genus Apodemus. Due to better storage conditions of foodstuff and targeted rodent control, this serovar is no longer as common as in the past. The main host of the serovars Icterohaemorrhagiae and Copenhageni is a rat, with which people living in poor social and hygienic conditions (including the homeless) often come into contact. There are currently many more such people in Slovakia than in the past.
Slight shift from the groups with professional exposure to non-occupational groups (groups without professional exposure or occupation at all) was noticed. At the turn of the 1950s and 1960s, the ratio was 57.8% vs. 42.2% in favour to professional exposure groups [12]. During our study period, the ratio was 74.38% vs. 25.62% in favour to non-occupational groups. People without professional exposure were mostly infected during gardening, cleaning garden sheds and barns, drinking water from unverified water sources or fishing. Slaughterhouse workers (1.66%) and farmers (5.77%) had the lowest representation among selected occupations in our study period and each of them were infected only by two types of serovars, former by Icterohaemorrhagiae + Copenhageni and Pomona, latter by Sejroe and Pomona [2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. Possible explanation can be a decline in the total number of workers in mentioned professions and reduction of human exposure due to mechanization of industrial production and better personal protection. Similar decline in number of leptospirosis of professionally exposed people was reported also from other industrialized countries (e. g. Germany, Italy, Israel, Netherlands), where leptospirosis has been common occupational disease mainly among agricultural workers, but the relevance of leptospirosis in the rural economy began to decrease [12, 21].
Proportion of leptospirosis by age is shifting over time and this shift is related to the changing activities of people of various ages. In the second half of the last century, many age groups were affected by leptospirosis with most of the cases in young adults and persons of productive age [12]. Nowadays, some age groups are affected less commonly or not at all, and majority of cases is in 20–69 years old persons with peak in 50–59 years old persons. Low occurrence or absence of infections in children and adolescents can be explained by spending less time in nature and near natural water areas and doing more indoor activities as compared to the past. While the increased agespecific incidence in the elderly people may be related to observed predominance of non-occupational risk exposure, which is largely independent of physical fitness or ability to work. Very similar results as ours come from Germany, where 80% of cases were 30–69 years old persons with the highest agespecific incidence in 60–69 years old people. The lowest was in children under 10 years old [21]. Studies from several countries pointed out, that leptospirosis affected mostly men of age 20–64 [15, 16, 17, 22, 24].
In the study of Costa et al. [16], the authors estimated that there are annually 1.03 million cases and 58,900 deaths due to leptospirosis worldwide and case-fatality rate of acute leptospirosis is 6.85%. Haake and Levett [19] concluded that case-fatality rate for leptospirosis varies from 5% to 40%. During our study period, two women and one man died due to severe icteric form of leptospirosis, therefore case-fatality rate was 2.48%. In Netherlands during longterm study (1925–2008), case-fatality rate for patients with reported leptospirosis was 6.5%, but the annual number of deaths decreased over time, probably because of improved treatment [18]. Even higher case-fatality rate was noticed in Ukraine, the average national case-fatality rate in 2005–2015 was 9.8% [23]. Low case-fatality rate in Slovakia can be explained by the fact that patients often receive antibiotic treatment immediately after the onset of symptoms, before the diagnosis is confirmed. Therefore, the disease is rarely fully developed before the patient receives the treatment. Fatal cases are predominantly untreated and uncooperative patients. In our study, all three fatal cases were patients living in poor social and hygienic conditions. They were unemployed, 30–41 years old people. Most of the cases during our study period were febrile infections (45.45%) with moderate course of infection (59.47%). Mild course of the disease had 19.01% of patients and severe course had 18.21% of patients. In the study of Zubach et al. [29] out of 395 patients only 2.3% had mild disease, moderate disease was observed in 27.3% and severe disease occurred in 70.4%.
The number of detected positive patients may be positively or negatively affected by the economic development of individual administrative region, the social and hygienic level of their inhabitants, the availability of the laboratory analysis (which is performed in Western Slovakia) and the number of samples sent for examination. The number of detected positive patients from individual regions differed. No part of Slovakia can be unambiguously described as high or low occurrence of leptospirosis.
Gender specific incidence and seasonality of human leptospirosis have not changed over time. The higher proportion of male cases persists, what can be explained by more frequent exposure of men to leptospires during professional and leisure time activities than women. The occurrence of human leptospirosis maintains a typical seasonal character. The highest proportion of infections was observed from June to November (77.73%). These findings are similar to seasonal occurrence in the 1950s [12]. Other countries in Europe have also recorded the highest distribution of leptospirosis in the same months of the year. This seasonal pattern can be explained by rainfalls, higher temperatures and increased number of rodents and small mammals in the warm months of the year in combination with leisure or occupational outdoor activities of people [17].
CONCLUSIONS
In 2008–2019, incidence rate of human leptospirosis maintains the declining character, which has been present in recent decades in Slovakia. Average annual incidence rate in the study period was 0.185/100,000 population and case-fatality rate was 2.48%. Although a decline in incidence rate can be explained, for example, by industrialization and changed lifestyle of population, we assume that incidence rate is underestimated and reflects mostly manifested infections. Leptospirosis remains a threat for human population, due to the existence of animal sources of infection. Consistent and systematic surveillance is therefore the basic tool for detection of the real burden and consequently effective control and management of this zoonotic disease.
Sources
- Abdullah NM, Mohammad WMZW, Shafei MN, et al. Leptospirosis and its prevention: knowledge, attitude and practice of urban community in Selangor, Malaysia. BMC Public Health, 2019;19(1):628. doi: 10.1186/s12889-019-6981-0.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2019. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2020.136 s. ISBN 978-80-972963-8-4.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2013. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2014. 128 s. ISBN 978-80-89738-00-7.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2014. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2015. 122 s. ISBN 978-80-89738-05-2.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2015. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2016. 116 s. ISBN 978-80-89738-08-3.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2016. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2017. 114 s. ISBN 978-80-89738-11-3.
- Antolová D, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2017. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2018. 118 s. ISBN 978-80-8143-231-6.
- Antolová D, et al. Summary report of zoonoses, their causative agents and water-borne diseases in the Slovak Republic in 2012. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2013. 120 s. ISBN 978-80-970552-9-5. 2013.
- Avdičová M, et al. Summary report of zoonoses, food-borne and water-borne diseases in the Slovak Republic in 2018. Bratislava: Ministry of Agriculture and Rural Development of the Slovak Republic; 2019. 126 s. ISBN 978-80-972963-4-6.
- Bakoss P, et al. Leptospiroses 2009−2011. In: Bakoss P, et al. Surveillance of zoonoses − leptospiroses, ornithosis, psittacosis and mammalian chlamydiosis. Bratislava: State Veterinary and Food Administration of the Slovak Republic; 2013. s. 6−62. ISBN 97880-7148-064-8.
- Bakoss P, Macháčová E, Jareková J. Long-term trends in the epidemiology of human leptospirosis (Slovak Republic, 1954 – 2006). Eur J Clin Microbiol Infect Dis, 2012;31(9):2167–2176. doi: 10.1007/s10096-012-1551-8.
- Bakoss P. Leptospiroses. In: Bazovská S, et al. Special epidemiology. Bratislava: Comenius University Publishing House; 2017. s. 328−336. ISBN 978-80-223-4179-0.
- Beauté J, Innocenti F, Aristodimou A, et al. Epidemiology of reported cases of leptospirosis in the EU/EEA, 2010 to 2021. Euro Surveill, 2024;29(7):2300266. doi: 10.2807/1560-7917. ES.2024.29.7.2300266.
- Ciceroni L, Stepan E, Pinto A, et al. Epidemiological trend of human leptospirosis in Italy between 1994 and 1996. European Journal of Epidemiology, 2000;16 : 79–86.
- Costa F, Hagan JE, Calcagno J, et al. Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl Trop Dis, 2015;9(9):e0003898. doi: 10.1371/journal.pntd.0003898.
- European Centre for Disease Prevention and Control, Leptospirosis. In: ECDC. Annual epidemiological report for 2015. Stockholm: ECDC; 2018.
- Goris MG, Boer KR, Duarte TA, et al. Human leptospirosis trends, the Netherlands, 1925–2008. Emerg Infect Dis, 2013;19(3):371–378. doi: 10.3201/eid1903.111260.
- Haake DA, Levett PN. Leptospirosis in Humans. Curr Top Micro biol Immunol, 2015;387 : 65–97. doi: 10.1007/978-3-662-450598_5.
- James S, Sathian B, van Teijlingen E, et al. Outbreak of Leptospirosis in Kerala. Nepal J Epidemiol, 2018;8(4):745–747. doi: 10.3126/nje.v8i4.23876.
- Jansen A, Schöneberg I, Frank C et al. Leptospirosis in Germany, 1962–2003. Emerg Infect Dis, 2005;11 : 1048–1054.
- Lara JM, Von Zuben A, Costa JV, et al. Leptospirosis in Campinas, São Paulo, Brazil: 2007–2014. Rev Bras Epidemiol, 2019;22:E190016. doi: 10.1590/1980-549720190016.
- Markovych O, Tymchyk V, Kolesnikova I. Leptospirosis in Zakarpattia Oblast (2005–2015). Vector Borne Zoonotic Dis, 2019;19(5):333–340. doi: 10.1089/vbz.2018.2356.
- Meites E, Jay MT, Deresinski S, et al. Reemerging Leptospirosis, California. Emerg Infect Dis, 2004;10(3):406–412. doi: 10.3201/ eid1003.030431.
- Mgode GF, Japhary MM, Mhamphi GG, et al. Leptospirosis in sugarcane plantation and fishing communities in Kagera northwestern Tanzania. PLoS Negl Trop Dis, 2019;13(5):e0007225. doi: 10.1371/journal.pntd.0007225.
- Mwachui MA, Crump L, Hartskeerl R, et al. Environmental and Behavioural Determinants of Leptospirosis Transmission: A Systematic Review. PLoS Negl Trop Dis, 2015;9(9):e0003843. doi: 10.1371/journal.pntd.0003843.
- Naing C, Reid SA, Aye SN, et al. Risk factors for human leptospirosis following flooding: A meta-analysis of observational studies. PLoS One, 2019;14(5):e0217643. doi: 10.1371/journal. pone.0217643.
- Yasouri SR, Moghadam RG, Ghane M. Identification of Pathogenic and Saprophytic Leptospira spp. from the Rice Fields of Tonekabon Township Using PCR Technique. Advanced Studies in Biology, 2013;5(10):437–445.
- Zubach O, Telegina T, Semenyshyn O, et al. Leptospirosis in Ukraine (Lviv Oblast): Clinical and Epidemiological Features. Vector Borne Zoonotic Dis, 2019;19(5):341–346. Bratislava: State Veterinary and Food Administration of the Slovak Republic; 2009. 22 s.
Conflict of interest
The authors declare no conflict of interest.
Do redakce došlo dne 31. 1. 2025.
Adresa pro korespondenci:
RNDr. Jana Perželová, PhD.
Ústav epidemiologie,
Lekárska fakulta Univerzita Komenského Bratislava
Moskovská 3
811 08 Bratislava Slovenská republika
email: jana.perzelova@fmed.uniba.sk
Labels
Hygiene and epidemiology Medical virology Clinical microbiologyArticle was published in
Epidemiology, Microbiology, Immunology

Most read in this issue
- Alternative nicotine delivery systems: current evidence
- Cancer screening in the Czech Republic
- Prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae in women of the Czech Republic armed forces
- Vaccination in pregnancy – a study in maternity hospitals of the Pilsen Region, Czech Republic