
The long-term monitoring of sympathetic ophthalmia in the diagnostic and terapeutic view. Review Department of Ophthalmology
Authors:
J. Krásný 1; T. Eckchlager 2; K. Smetana 3; J. Šach 4; H. Šubrtová 5
Authors‘ workplace:
Oční klinika FN Královské Vinohrady a 3. LF UK, Praha, Přednosta: prof. MUDr. P. Kuchynka, CSc.
1; Dětská onkologická klinika FN Motol a 2. LF UK, Praha, Přednosta: prof. MUDr. J. Starý, DrSc.
2; Ústav hematologie a krevní transfuze, Ředitel: prof. MUDr. P. Cetkovský, Ph. D.
3; Ústav patologie, FN Královské Vinohrady a 3. LF UK, Praha, Přednosta: prof. MUDr. R. Matěj, Ph. D.
4; Hematologická klinika FN Královské Vinohrady a 3. LF UK, Praha, Přednosta: prof. MUDr. T. Kozák, Ph. D, MBA
5
Published in:
Čes. a slov. Oftal., 75, 2019, No. 5, p. 235-248
Category:
doi:
https://doi.org/10.31348/2019/5/1
Overview
Aim: To evaluate options of diagnostic and therapeutic procedures of sympathetic ophthalmia (SO) compared with literature data.
Backgroud: SO is an ocular autoimmune disease. It is characterized by disbalance in the imunoregulatory T-subsets within cell mediated immune response.
Methods: File examination of SO by evaluation humoral and cellular immunity was ranked nukleolar test (NT). It evaulates the current status of lymphocyte activation based on the nucleolar morphology and RNA transcription aktivity. The classical histological examination was supported by immunohistochemical analysis of lymphocytic subpopulations in the eyeball enucleated for. SO in one case.
Material: Five boys and men overall were monitored and treated in two studies from 1979 to 1994 and from 1999 to 2017 with SO In four cases it was subsequent after penetrating injuries and once after lensectomy with vitrectomy. The age of patients in the time of onset of SO was between 4 and 24 years (average 12 years). The time interval between insult and onset of SO varied between 10 days and 3 months (average 1.7 months). The relaps of disease appeared in the all cases in the time interval from 3 months to 38 years (average 15 years). Another two patients with SO were examined only in consultation: 16 years old boy with relaps of SO after cataract extraction and 71 years old women with SO subsequent after lensectomy and vitrectomy. There was examined and compared group of 19 patients with other types of uveitis in the same time. The lens-associated uveitis were caused after ocular contusion and penetrating eye injury in 16 patients (13 male patients). In another three cases (young women) with uveitid underlined by II. or III. type of hypersenzitivity the enucleation of dolorous eyeball calmed down the secondary uveitis on their second eye without any change of immunosupressive treatment and without change in NT.
Results: There were changes in the complex immunological laboratory tests results in the SO cases in the counts of activated lymphocytes in the peripheral blood. The count of activated lymphocytes was increased in SO cases unlike in lens-associated uveitis. There was detected in NT statistically significant difference (p = 0,0134) between the two groups of uveitis. The histological examination (5 eyes with SO and 7 eyes without sympathetic uveitis) confirmed the diagnoses, supporting basically the clinical diagnosis. The immunohistochemical examination corfirmed the presence of populations of T-lymphocytes, macrophages and also B-lymphocytes. A basis of immunosuppressive therapy was the combination of prednisone and azathioprin at the first time. Effective therapy featured cyklosporine later.
Conclusion: The nucleolar test of lymphocytes draws attention of their up-to-day increased activity without the diferentiation of subpopulations and their absolute number increase related to the current activation of type IV. hypersensitivity (cell-mediated) in uveitis mechanism. The immunosupressive therapy calmes down this activation predominantly in SO, but also in other case sof uveitis with different types of hypersensivity. The immunohistochemical examination illustrates different presence of lymphocytic types according to the stage of SO.
Keywords:
Sympathetic Ophthalmia – Functional Lymphocytes Activity – immunosuppressive therapy – Lens-Associated Uveitis – Transcription of RNA
INTRODUCTION
The sympathetic pathology ophthalmia sympatica, or sympathetic uveitis (SO), is a bilateral diffuse granulomatous uveitis. After injury to the uveal tissue following an injury, surgical procedure or as a result of other therapeutic procedures an inflammation occurs in the exciting and initiating (i.e. “sympathetic” according to the academic Kurz) eye, and after a period of time “sympathetic” uveitis appears also in the previously healthy eye (sympathising eye) (47). Its characteristic image features fatty precipitates on the endothelium (Fig. 1B) and yellowish-white nodular lesions of the choroid, termed Dalen-Fuchs (D-F) nodules (Fig. 1C) (14), the frequency of which is within the range of 25% to 35% (51). In its mechanism, SO ranks among pathologies of type IV hypersensitivity, i.e. Cell-Mediated Immune Response (CMI). A sensitised lymphocyte following an encounter with an antigen (at least three are considered) begins to produce mediators, interleukins. These low-molecular peptides act on further lymphocytes or cells capable of transmitting information for the relevant immune response. Among these, an especially important role is played by two factors, namely inhibiting macrophages and activating macrophages. These later attack the vascular wall, together with various sub-populations of lymphocytes, including NK (Natural Killers) of cells penetrating into the uveal parenchyma (Fig. 1A) together with other cells of the immune response. In the next phase there follows formation of immense epithelioid cells and inhibition of granulocytes. The stimulation of lymphocytes under the influence of interleukins leads in the final phase to damage to the intraocular tissues, mainly the uvea and retina, either by lymphotoxin, or contact-dependent cytolysis (34, 47). Lymphotoxin represents one of the cytokines: TNF-beta with necrotising effect suppressing cell growth, at the same time with anti-inflammatory effect, and contact-dependent cytolysis is then a non-specific immune response of the present NK cells leading to osmotic lysis of the target cells (26).

Long-term observation of SO together with an analysis of the data from the literature has enabled us to assess the development of therapeutic procedures, but above all to consider the possibilities of laboratory observation of the immunopathological character of this disease in defining the nature of the inflammatory process in the eye.
METHOD
In order to observe the dynamics of SO we included a broad spectrum of laboratory examinations from the peripheral blood, conditional upon the given time. In the spectrum of humoral immunity we evaluated the immunoglobulins IgA, IgM, IgG and circulating immune complexes PEG. We assessed cellular immunity together with the blood count, the originally used E-rosettes (total number of T-lymphocytes) or immune regulation index (ratio of absolute number of helpers to cytotoxic T-lymphocytes in peripheral blood) were replaced by individual sub-populations of lymphocytes (CD3, CD4, CD8, CD20, CD56 etc.). Within the autoantibodies we included those that have a relationship of uveitis to general autoimmune diseases (ANA, ANCA, anti ds-DNA, ENA) and from serology this was ASLO. We independently assessed a nucleolar test (NT), which represents a method enabling evaluation of the current state of biosynthetic activation of lymphocytes on the basis of the nucleolar morphology. For highlighting of nucleoli in lymphocytes we used cytological staining of peripheral blood smear by 0.05% toluidine blue at pH 5 for demonstration of RNA according to professor K. Smetana (67, 68, 69, 71, 72). Lymphocytes can be divided into three types according to the functionally dominant type of nucleolus (Fig. 2):
- The most widely represented are lymphocytes with a ring nucleolus (R), which is illustrated in the form of a dark ring in the nucleus. It contains ribonuclear protein structures only in the periphery of the nucleolus, and is referred to as a “pacific nucleolus”. The cells have a low level of r-RNA synthesis, but are capable of further activation and may contain micronucleoli.
- Activated lymphocytes (A) with an “activated nucleolus”, visible as a compact homogeneous oval in the nucleus with relatively uniform distribution of RNA, distinguished by high transcription of RNA. These are cells producing interleukins, which influence the cells capable of immune reactions or cells of the early phase of blastic transformation.
- Lymphocytes only with micronucleoli (M) have nucleoli which appear as dark points in the nucleus of the lymphocytes. Micronucleoli (inactive nucleoli) are nucleoli smaller than 1.2 µm and appear as small, round particles of ribonuclear proteins. This concerns the terminal stage in the development of lymphocytes which are no longer capable of further activation and their number is influenced by the increased turnover of lymphocytes. In an optical microscope inverted to 800x enlargement the proportion of activated lymphocytes and cells with micronucleoli out of a total number of 100 sought lymphocytes is calculated, in which the remainder is formed by inactive lymphocytes with a ring nucleus, which is expressed in percentages (the numerical data is presented in the text after symbols of three types of lymphocytes). Between the second and twelfth year of life the referential values of the nucleolar test for activated lymphocytes are within the range of 4-7% and lymphocytes with micronucleoli between 8-14%. These values decrease slightly at a higher age.

Immunohistochemistry is a new method used in histology, which on the principle of antigen-antibody binding can identify any substance with antigen properties in histological cross-sections, e.g. it differentiates sub-populations of lymphocytes. The method is composed of three fundamental phases:
- application of primary antibody (formation of immune complex),
- application of secondary antibody (generation of enzymatic activity of formed immune complexes)
- administration of detection system (colour indication of antigen in cross-section) (63).
Own cohort
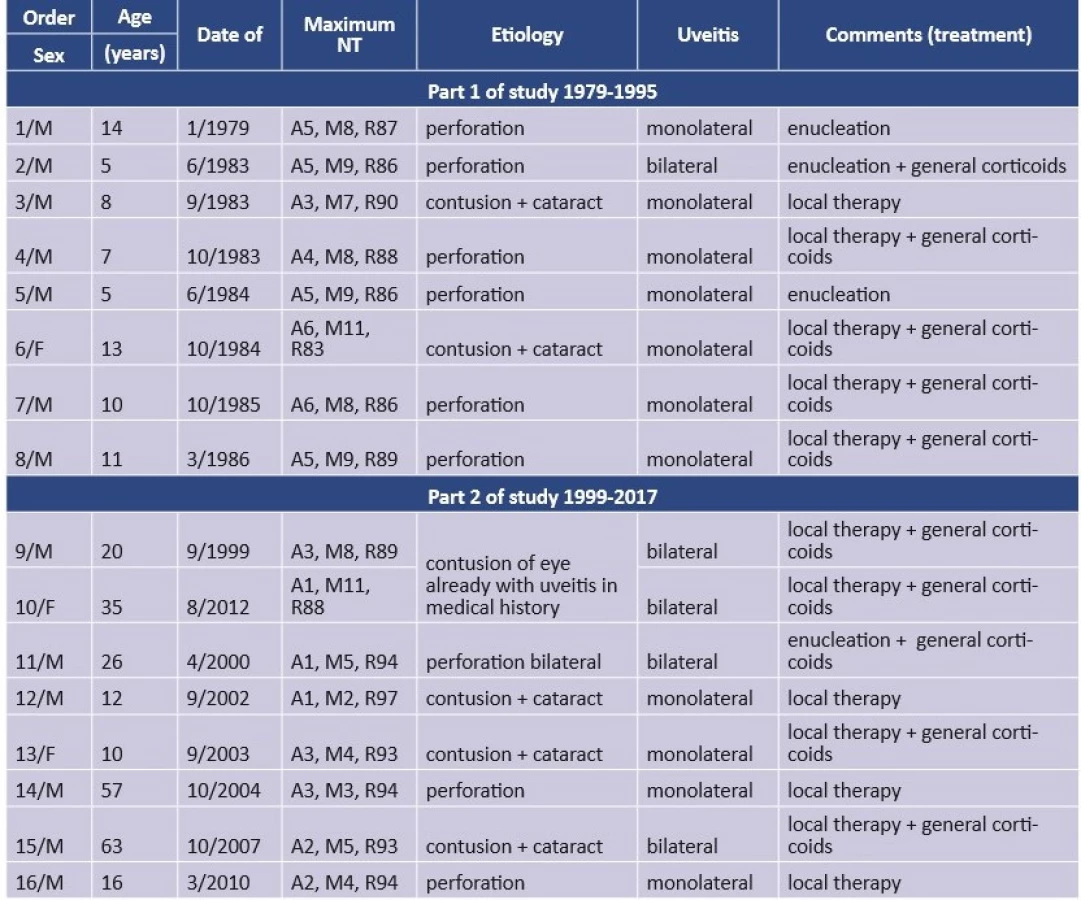
Observation of SO took place within two periods of time, covering a total period of thirty-five years. Table 1 presents the time factors of the development and course of five patients with SO, the forms of general immunosuppression, complications and the clinical finding at the end of the study. Table 2 primarily analyses NT within time contexts, HLA typing and the fundamental immunological parameters of cellular immunity, and according to the possibilities at the given time for SO. Table 3 presents the NT values together with etiology and treatment in 16 cases of post-traumatic phacoantigenic uveitis.


Part 1 of the study was part of the research project IGA 1152-3 (1994-1994) (46) in the years 1979-1994, covering observation and treatment of 3 boys with SO between the ages of 6 and 15 years (Table 1). At the same time we conducted a consultation examination on a further 16 year old male patient with SO. We also compared the laboratory values with a group of 6 patients (aged 5-14 years, average 9.1 years) with post-traumatic uveitis of non-inflammatory etiology – phacoantigenic (phacoanaphylactic) and their treatment (Table 3).
Part 2 of the study took place from 1999 to 2017, when the observation related to 2 new adult patients with SO and 2 now adult patients taken on from part 1 of the study, and with a laboratory evaluation for 10 predominantly adult patients (12-63 years, average 28.4 years) with post-traumatic uveitis, as well as subsequently exacerbated uveitis of non-traumatic etiology in three young women, including therapeutic procedures (Table 3). This included a consultation examination of an enucleated eyeball in a 71 year old woman also with regard to the immunohistochemical aspect.
An evaluation of five patients with SO (Table 1) was conducted on four boys and one young man (average age 12 years). The cause was perforating injury or contusion-laceration injury, in which SO originated on average 2 months after the trauma with the occurrence of inflammation of the sympathising eye in 3 of them due to enucleation of the exciting and initiating eye. In only one case SO developed in the second eye 1 week after enucleation of the blind and irritated eye (patient two and Fig. 1BC). The cause of origin of SO 10 days after lensectomy with vitrectomy due to congenital cataract with persistent hyaloid artery in a boy with Down’s syndrome (patient 3). In this patient relapse of the pathology occurred following initial alleviation of the inflammation after 3 months, upon reduction of immunosuppression. The parents refused the proposed application of cyclophosphamide (CYC) and transferred to another centre. The subsequent fate of the patient is unknown to us.
In November 1986, we conducted only a consultation examination on a 16 year old patient who was without immunosuppressant therapy. SO in the left eye developed at the age of six years following a corneoscleral injury in the right eye. Histological verification of the enucleated eyeball is not available. Extraction of a cataract in the left eye was performed outside of the territory of former Czechoslovakia 3 years after the inception of SO. Seven years after cataract surgery the left eyeball was hypotonic and the pupil was fixed to a secondary membranous cataract with a speculum and the vitreous body was opacified (Fig. 3A). Visual acuity (VA) in the left eye was 1.5/50, for near vision Jaeger (J) no. 13 with aphakic correction. NT demonstrated pronounced activity: A11, M7, R82. Prednisone 2 mg/kg and azathioprine 2x 50 mg daily were applied. VA in the left eye was stabilised at 2-3/50. The subsequent fate of the patient is unknown.

A relapse of this autoimmune disease following discontinuation of immunosuppression was manifested in three out of five patients from the observed groups within the range of a few months to a number of decades. The longest period of remission was 38 years after the origin of SO in a boy then aged 4 years old, in whom enucleation was performed at another centre in 1964 following manifestation of SO in the other eye (verification of SO was conducted at our centre). In a patient with Down’s syndrome, relapse of SO by means of vitritis (Fig. 3B) occurred upon reduction of a single dose of immunosuppressant, and also occurred in a young man with manifestation of SO on a maintenance dose of immunosuppressant of 20 mg of prednisone every other day. In this patient 4, the relapse was preceded two years previously by a slight increase in the activity of the inflammation (intimation of flare and isolated cells on the endothelium in the form of a Lüsse line), which was resolved only by parabulbar application of triamcinolone 40 mg (Kenalog, Léčiva). A complication in all patients in the sympathising eye was cataract and in three cases secondary glaucoma. Complicated cataract initially developed in the form of posterior subcapsular cell-like forms also a consequence of general corticosteroid therapy. This remained in patients 1 and 4 without any significant influence on vision. In a further two patients cataract gradually progressed: patient 2 and patient 5 (Fig. 3C). It was necessary to proceed to a surgical solution due to VA in the right eye of 0.05 and 0.02 respectively. The progression of such a pronounced deterioration of vision was influenced by waiting for absolute clinical and laboratory pacification of SO, which enabled a phacoemulsification technique with implantation of a posterior chamber intraocular lens (PC IOL) with perioperative immunosuppressant treatment by Solu-Medrol and an increased dose of cyclosporine A (CsA) in 2005 and 2003 respectively. Secondary glaucoma was manifested in 3 patients. Conservative therapy managed to normalise it in two cases (patients 1 and 5). Only in patient 2 this treatment was ineffective, and so in 2011 the condition was compensated with the aid of a glaucoma implant Express 100 (Alcon), which subsequently enabled the discontinuation of therapy with local anti-glaucomatous agents (Fig. 1D). The longest remission time of three decades was recorded in patient 1, who is without maintenance immunosuppression in the long term, has ceased to attend follow-up examinations and has remained in contact only by telephone. In a further two patients the maintenance treatment by a dose of CsA remained at less than 1 mg per day. This concerned individuals who had undergone a surgical solution of complications. In both patients, transitional activity was manifested on the anterior segment of the eye in the postoperative period, despite an increased dose of CsA, without vitreous reaction. In patient 4, who in 2014 underwent amputation of a leg due to post-traumatic phlegmon, we changed immunosuppression before this operation. We replaced prednisone together with azathioprine by CsA. In the postoperative period only a Lüsse line of cells appeared on the corneal endothelium without flare in the anterior chamber, without progression of cataract (Fig. 3D). After almost one year we were forced to replace the maintenance immunosuppression by CsA with the original treatment due to the patient’s constant intolerance (nausea).
We assessed 16 phacoantigenic (phacoanaphylactic) predominantly unilateral cases of uveitis (Table 2) following perforating injury or less frequently following contusions with rapid onset of intumescent cataract. Here there was a clear predominance of the male population over women in a ratio of 13 : 3. A bilateral inflammatory process following unilateral perforating injury was detected only twice (patients 2 and 15). Contusion of the eye with intraocular inflammation in the medical history was generated by secondary irritation also in the other hitherto healthy eye also in two cases (patients 9 and 10). Enucleation was designated according to the clinical condition of the eye and its prognosis. General immunosuppression by corticoids was always indicated in the case of bilateral processes, but also in the case of pronounced clinical manifestations of unilateral incipient uveitis.
Two young women were included with pauciarticular form of juvenile idiopathic arthritis (JIA) with ANA+ at pre-school age, in which bilateral uveitis preceded manifestations in joints. The joint and ocular process was progressively successfully stabilised by general immunosuppressant therapy: prednisone, later azathioprine and methotrexate (MTX) up to the use of CsA and CYC. Later, at the age of 16 and 23 years respectively, despite all medical efforts, unilateral secondary glaucoma occurred and changed in dolorous form in the eyeball turning blind. This change triggered secondary irritation in the other eye with already original long-term remission of uveitis upon a background of JIA. After enucleation of the blind eye at the age of 30 and 26 years respectively, uveitic irritation in the other eye subsided upon application of the same therapy as before the mutilating procedure, and vision was stabilised at VA 0.5-0.66 with correction. We observed the third patient from the age of six years (1998-2006) due to bilateral iridocyclitis with vasculitis of the retina and central non-parasitic granulomatous chorioretinitis afflicting the region of the optic nerve in the left eye. Due to persistent mild activity of uveitis in the right eye we temporarily did not recommend solution of complicated cataract, and in January 2006 we transferred the patient from prednisone to CsA. The patient’s parents themselves decided to seek medical care at another centre, where lensectomy with vitrectomy was performed in the right eye. At the age of 13 years bevacizumab (Avastin, Genentech) was repeatedly applied intravitreally. In May 2007, the patient returned to our medical care after an interval of one year due to bilateral exacerbation of panuveitis without general therapy. In the right eye the patient had hypotonia and VA of light perception with imprecise projection (Fig. 4A). In the left eye the patient had flare in the anterior chamber with seclusion of the pupil to the opacified lens and VA of 0.05 natural (Fig. 4B). We repeatedly commenced immunosuppressant therapy using CsA with the aim of stabilising the inflammation in the left eye and saving the right eye. In May 2008 we proceeded to enucleation due to constant inflammatory activity in the right eye with mild inflammatory irritation also in the left eye. In October 2010 the patient underwent cataract surgery in the left eye with implantation of a PC IOL, with immunosuppressant treatment with a combination of Solu-Medrol and CsA. We secured subsequent release of the seclusion and YAG capsulotomy in October 2013 with tacrolimus (Prograf, Astellas Pharma) for CsA. In November 2017 the inflammation was still in remission upon maintenance therapy of CsA 1 mg/kg/day. VA in the left+ eye was 0.15 with -3.0, near VA J. no. 6 naturally was conditional upon changes on the ocular fundus (level of baseline VA from 1998).

RESULTS
In total NT was used 87 times on patients with SO and approx. 60 times on patients with non-sympathetic etiology of uveitis (only patients with at least twice conducted NT were included). Table 2 presents the results of NT in the case of SO at the beginning of observation, its highest value and the last examination within the framework of the study. NT was always increased for all 3 child patients upon the initial detection of SO and for an adult patient upon relapse without immunosuppressant therapy (patient 5). Whereas the test was initially within the norm in patient 4 within the framework of immunosuppression, despite this mild immunosuppression a relapse of SO triggered its pathological increase. The highest maximum values of NT were manifested upon a relapse of the pathology in patient 2 and primarily in the 16 year old patient treated by consultation, always without general immunosuppression. It was only during the course of this aggressive general immunosuppressant therapy that the NT values always progressively decreased, as was demonstrated also by the last examination in 4 of them. This was confirmed also by the transitional decrease of NT in patient 3 to the NT value: A5, M16, R79 with subsequent increase upon an endeavour to reduce immunosuppression. The values of the sub-population of T-lymphocytes CD4 in peripheral blood were reduced at the time of maximum activity of NT in two patients, and increased in another two patients (within the framework of evaluation of E-rosettes). Only in one case was the number of CD4 increased and CD8 reduced (patient 6). Observation of sub-populations of lymphocytes or their analogy determined by the time of examination (immune regulation index) during the course of SO did not demonstrate significant values. Examination of humoral immunity and autoantibodies was always negative.
No pathological NT value was detected in the case of phacoantigenic (phacoanaphylactic) uveitis in any of the cases (Table 3), in which NT was slightly below the borderline values in two cases (patients 6 and 7). The uveitic process was always definitively suppressed by local and if applicable also general treatment with corticoids to NT values within the range of: A2-3, M5-7, R91-94. This dynamics of the process attested to the minimal presence of lymphocyte activity in this type of intraocular inflammation. Minimal NT activity was linked with immunosuppressant therapy in two patients with JIA uveitis, which was beneath the referential values, upon therapy with CsA and MTX NT was: A1, M6, R93, and upon a combination of Medrol with CYC NT manifested: A0, M7, R93. The influence of immunosuppression was demonstrated also by a change of therapy in a 14 year old girl following lensectomy with application of bevacizumab – before and after application of CsA, NT decreased from A5, M5, R90 to A1, M7, R92, and upon transition of the maintenance therapeutic dose of CsA to securing treatment by tacrolimus NT decreased from A2, M3, R95 to A0, M4, R96. We conducted a statistical evaluation comparing the maximum values of NT at the time of the highest clinical activity of SO and acute phacoantigenic uveitis (only values of patients without any immunosuppressant therapy). A two-step T-test demonstrated significant differences in active lymphocytes on a statistical level of significance (p = 0.0134), despite the fact that it was not possible to exclude the possibility of error of small numbers. The evaluation of lymphocytes with micronucleoli (p = 0.5426) and inactive ring lymphocytes (p = 0.1333) was not statistically significant.
Histological verification of seven enucleated eyeballs, which did not confirm SO, was of fundamental importance in a 14 year old patient following the application of bevacizumab. Above all cicatricial changes were confirmed, specifically an atrophic and fibrotised ciliary body and an irregularly convoluted detached retina (Fig. C4) with gliosis and post-inflammatory atrophy and fibrotisation of the choroid (Fig. 4D). In this uveitis, with regard to the preceding type of operation it was possible to assume co-participation of type II cytotoxic mechanism of hypersensitivity. This image of cicatricial changes without floridly progressing granulomatous inflammation was detected in the enucleated eyeballs of both young women with JIA uveitis. It is possible to assume that this concerned a type III immune complex mechanism of hypersensitivity characteristic for JIA, and not type IV hypersensitivity.
Histological verification of an eyeball examined by consultation in a 71 year old woman, in which SO originated following vitrectomy performed due to vitreoretinal proliferation, confirmed this pathology. The retina was with chronic total detachment, entirely disorganised and severely gliotically altered. In the connecting subretinal proliferations and also in the uveal tissue itself there were inflammatory deposit infiltrates formed predominantly by lymphocytes and macrophages (Fig. 5A) with pronouncedly dominant T-lymphocytes (Fig. 5B). Immunohistochemically (Fig. 5 below) there were positive sub-populations of CD3, but also CD4 with CD8. The minority part of the infiltrate was formed by B-lymphocytes CD20. In the infiltrate there was relatively abundant participation of macrophages positive for antibodies CD68, which bordered the Dalen-Fuchs nodules.

CONCLUSION
NT draws attention to the current increased activation of lymphocytes, without differentiation of the representation of sub-populations and their absolute number in the mechanism of uveitis in type IV hypersensitivity. Immunosuppressant therapy fundamentally influences this activity by means of a decrease in values, primarily in SO, but also of uveitis of other types of hypersensitivity. Immunohistochemical examination demonstrates various representation of individual types of lymphocytes according to the stage of SO.
DISCUSSION
A nucleolar test was included in the points system of haematological examinations of the General Health Insurance Company in the Czech Republic under code 91467, and is still valid. This examination was previously used in the case of pathological conditions in which there is a contribution of late cellular hypersensitivity. The reaction of the graft to the host following transplantation of bone marrow (30) and in relation to rejection of kidney grafts (44) was accompanied with an increase in the number of activated lymphocytes. This fact was the reason for our inclusion in the range of laboratory immunological examinations in the case of our patients with SO. This concerns an examination connected with the name of the Czech haematologist, professor K. Smetana, when its precise rules were stipulated during the course of the 1960s and 70s (67, 68, 71). Chronic lymphocytic leukaemia in advanced stages was accompanied by an increase in the number of active nucleoli, and subsequent chemotherapy reduced their number (73), as confirmed by the ultrastructure of the nucleoli (70), which is a parallel to the decrease of active lymphocytes in SO upon immunosuppressant therapy of our patients and upon maintenance doses of these medications, which was confirmed also in the case of other medications (21). An increase in the number of active nucleoli was demonstrated in the case of systemic pathology of conjunctival tissue (44) in connection with activity of joints in JIA and rheumatoid arthritis in adults (77). In our patients, in whom uveitis was linked with JIA, with only ocular symptomatology, increased activity of nucleoli in lymphocytes was not manifested also with regard to immunosuppression. The increase of nucleoli in lymphocytes of the peripheral blood was demonstrated in persons who liquidated the disaster at the nuclear power plant in Chernobyl as a cytogenic radiation effect (32). At present the use of NT for autoimmune diseases and blood tumours has been surpassed due to a through-flow cytometer distinguishing individual sub-populations of lymphocytes in peripheral blood. Furthermore, proliferation markers Ki67 (MiB1) distinguish the ongoing cellular cycle of cells in the phase of mitosis and preparation for it. Despite this, NT can provide new observations, also in the field of other types of uveitis.
Sympathetic ophthalmia in Czechoslovak ophthalmology first appeared within the period of 1927-1932, with regard to the authors of six articles it is possible to name distinguished ophthalmologists such as professor Záboj Bruckner: Ophthalmia sympathica in luetico following perforated serpiginous ulcer (10) or professor Václav Vejdovský: Sympathetic ophthalmia following cataract surgery (80). After the Second World War there was an endeavour to treat SO with the aid of penicillin, which at that time was considered causal (19). The first immunosuppressant treatment of this disease in Czechoslovakia was described in 1958 with the aid of adrenocorticotropic hormone (ACTH) and prednisone (38). In the case of a 17 year old girl, treatment was conducted by means of the above-stated immunosuppression and without enucleation of the injured eye (39). A study of four patients always addressed the condition of the injured eye upon generation of SO by enucleation. The author supported the infection-allergy theory of the origin of SO, and as a result the patients were treated generally with prednisone and antibiotics (57). Relapse of SO was triggered by an endeavour to release seclusion of the pupil by corepraxis (with the aid of photocoagulation technique) (35). Timely and effective immunosuppressant therapy in a combination of azathioprine and prednisone enabled saving of the eyeball and the performance of reconstructive surgery on a 17 year old patient (17). The last hitherto published study now deals with the issue of SO as a consequence of pars plana vitrectomy in two patients out of four observed, in which prednisone was therapeutically selected, or in a combination with MTX or CsA, without enucleation (75).
With regard to the fact that 13 years have passed since this last study and SO still receives substantial attention from ophthalmologists at present (PubMed), we have also included an analysis of the literary data.
Historical view of sympathetic ophthalmia. It is assumed that SO was the subject of study already in the times of Hippocrates. The first written report was recorded by Constantius Cephalis in approximately 1000 BC: “The affected eye frequently transmits its suffering to the other” (20). The clinical picture of SO was first described in book form in Greek in the 16th century: “After injury of the right eye, the left eye was also subsequently severely affected” (8). The actual term “sympathetic” illness was first used by MacKenzie in the 19th century (52). At the beginning of the 20th century Pusey expressed a hypothesis concerning the hypersensitive character of the pathology (60). The theory of the origin of SO was focused on by two historically celebrated ophthalmologists; professor Fuchs described nodular infiltration of the uveal tract (25), and professor Elschnig considered the antigenic property of uveal pigment to be the cause of the pathology (22).
Etiology of sympathetic ophthalmia. An American study of SO from the period of 1913-1978 on 105 patients, with a predominance of men (67%), was conditioned primarily as postoperative complications of then-performed intracapsular extractions of cataracts in 28% of cases, despite the fact that there was a general predominance of penetrating injuries in the etiology (53%), and at the same time SO was also described in the case of severe contusions of the eye (51). In a more recent Indian study from the turn of the 21st century the representation of men was similar, 62% of 130 patients with SO, and its etiology was post-traumatic in 3/4 of cases (78), which corresponds to observations from the 1980s (13). A summary overview of Czech and Slovak studies from 1958-2017 shows 89% representation of men and 73% of injuries out of 19 observed patients. The annual incidence of SO at the end of the last century decreased to 0.03 per 100 000 of the population (41). The danger of onset of SO following a penetrating injury is within the range of 0.1 to 0.3%, whereas in ocular surgery overall it is only 0.02% (56). At the end of the last century SO was described in isolated cases following cataract surgery, in the initial stages of implantations of intraocular lenses (79). A far more serious risk is represented by vitrectomies with an incidence from 0.06% (28) to 0.97% (32); at present these are primarily reoperations with a frequency of 0.125% (3), and in the case of retinal surgery in 0.37% (33). The most numerous and latest cohort of 175 patients with SO from the Commonwealth states only 16 cases of SO following vitrectomies (9%) out of a total number of 41 365 of these operations, which means that the risk is now only 0.038% (80). SO following vitrectomies has been recorded twice also in this country (75). In the case of a procedure without breaching the corneoscleral limbus of the eye there also still remains a danger of occurrence of SO. It has occurred upon YAG cyclotherapy of glaucoma (4, 50), in which the incidence of SO decreased from 5.8% in the 1990s (49) to 0.03 to 0.17% (4) in this century. SO may originate also following brachytherapy of melanoma (1, 24) or proton therapy (8) and its resection (29). Furthermore this tumour may trigger the onset of SO through its growth (51, 56). In rare cases the onset of SO has been observed following the application of a filling in extraocular retinal surgery (58). SO has originated following perforation of a corneal ulcer, triggered by chemical burn (65), as well as following other stimuli (51). Recently SO has been recorded following anti-VEGF therapy, due to the influence of intravitreal application of bevacizumab (9, 66).
Time factor of onset of sympathetic ophthalmia. The severity of SO consists in the fact that it can occur even several years after the ocular trauma (14, 54, 51); in the literature the range is stated at from 5 days to 66 years (14). Isolated cases of SO have already been described previously (2%) with confirmed histological verification manifesting shortly after enucleation (16, 51). This was also confirmed by a later study in 5 to 7% (14). We detected this in one patient. The most frequent and initial symptoms of SO are a deterioration of vision in 89% accompanied with pain in 29% and vitreous opacities in 24% (78), as well as ciliary injection and photophobia (76).
Laboratory verification of sympathetic ophthalmia. The pathology is stated as bilateral granulomatous uveitis, characterised by a pronounced proportion of T-lymphocytes in the inflammatory infiltrate of the choroid together with macrophages (14, 63), which are decisive for the histological diagnosis. This corresponds to the theory of type IV hypersensitivity, in which SO served as its model in the 1980s (34). Immunohistochemical studies in further years revealed new facts, since D-F nodules contain T-lymphocytes, mainly CD4 (helpers) and CD8 (suppressors or cytotoxic cells) in a ratio of 3 : 1 to 4 : 1 (later the proportion is reversed). NK cells are diffusely throughout the entire choroid. There is also presence of a small quantity of B-lymphocytes in the acute phase (11, 14). Moreover B-lymphocytes were detected in a larger number in D-F nodules in two out of four enucleated eyeballs (5). Later it was detected that the number of macrophages and B-lymphocytes may be higher than T-lymphocytes in different phases of SO (6) in the final phase of SO, when B-lymphocytes reactivate T-lymphocytes (17). More detailed detection showed that in the first phase of SO granuloma of D-F nodules contain M1 macrophages (CD68, CD 163) than other T-lymphocytes. The PCR (polymerase chain reaction) method detected only specific cytokines in the nodules (IL-7, IL18, IL-20, CCL19 and CXL11) (27). With regard to NT positivity in blood tumours with a pronounced representation of B-lymphocytes (73), it ensues that for the activity of NT in SO it is not decisive as to whether this concerns T - or B-lymphocytes and their absolute value, but what is of fundamental importance is the overall biological activity of all lymphocytes. Neither analysis of the information over several decades on the information portal PubMed, nor several fundamental studies on SO in their conclusions and detailed discussions in recent years (3, 16, 17) have provided information about the possibilities of monitoring SO upon evaluation of sub-populations of lymphocytes in peripheral blood. Levels of T-lymphocytes are described as variable (23, 56) or a decrease of sub-population CD4 and the thus ensuing change in the immune regulation index (54). This was confirmed by its decrease upon examination in two of our patients. A decrease of T-lymphocytes was demonstrated in peripheral blood in correlation with an increase thereof in uveal tissue (37). None of these examinations of levels of lymphocytes in peripheral blood are of a dynamic character, because SO does not have systemic manifestations. In the SD-OCT image D-F nodules manifest hyperreflexive lesions in RPE with impairment of the transition of internal and outer layers of fibres (53).
Pathogenesis of sympathetic illness. It is also considered that a histocompatible code of those affected applies within the etiology of origin of the pathology. A higher incidence of the antigen A11 (14, 62) was determined, which we confirmed in one patient. The antigen B27 may also have a certain significance (62), confirmed in another of our patients. Of other predisposing antigens these are B40 and DR4/DRw53 or DQw3 (14), later other antigens HLA-DRB1 and DRQA1 were stipulated in the white population (42). In seeking the etiological causes of SO a direct relationship was detected with Vogt-Koynagi-Harada (VHK) syndrome, characterised by uveo-menigoencephalitis and uveo-cutane syndrome. Both pathologies are accompanied by similar bilateral granulomatous uveitis with extensive infiltration of the choroid, conditioned by a T-lymphocytic reaction to an uveal retinal antigen (60), characterised as an autoimmune disease with immunological dysregulation (2) and certain common HLA antigens, specifically DR4 and DRW53 (12). VKH syndrome in its initial stages is manifested in a decrease in T-lymphocytes, primarily of sub-populations of CD4, but also CD8 (49), which we confirmed by means of a decrease of overall T-lymphocytes in two boys (48). In the later stages of the pathology there was an equalising to rise of T-lymphocytes (12, 48, 49). From this it ensues that observing the level of T-lymphocytes in peripheral blood in VHK syndrome enables its monitoring, unlike SO. No exact experimental model of SO exists yet, but in monkeys it was possible to develop uveitis with D-F nodules by the antigens IRBP and S-A (54). New types of experimental autoimmune uveitis in animal models demonstrated the influence of cytokine dysregulation and mitochondrial oxidative stress. Precisely in the case of SO, the influence of photoreceptor mitochondrial damage is considered (55), and here also the influence of TNF-alpha, leading to apoptosis of photoreceptors, is considered (17). An autoimmune reaction is assumed against the originally sequestered retinal antigen (S-Ag) or inter-photoreceptor retinoid-binding protein (IRDP) or rhodopsin (16). Cellular immunity has also been evaluated, e.g. blastic activity or lymphocytic transformation (23). A new strategy of treatment could be represented by synthetic preparation of microRNA. Identification of change in the level of microRNA upon its expression profiles the possibility of a new view of the pathogenesis of SO, because in the case of this disease a number of specific microRNA have been detected, which are used as a regulating medium in activation of lymphocytes. Both methods, namely the American (36) and Czech (67, 68, 71) focus on changes of lymphocyte activation. The American method of the study uses molecular genetic analysis based on PCR (36), whereas the Czech method of professor Smetana (67, 68, 71) is morphological work with the aid of microscopic laboratory examinations. They are linked only indirectly, but a certain correlation exists. This concerns verification of the state of RNA transcription in the nuclei of the lymphocytes influencing their biological activity.
Therapy of sympathetic ophthalmia. In treatment of SO, whether with or without enucleation of the exciting and initiating eye, general immunosuppressant therapy is applied, which is the most economically demanding of all uveitis (45). In addition to corticosteroids in high doses, which still form the basis of therapy (14, 23, 54, 56, 75), we applied mainly at the beginning. Later other immunosuppressants and cytostatic drugs were included: azathioprine, CYC, MTX, mercaptopurine (14, 23) or high doses of chlorambucil (59), in combination with mycophenolate in the case of refractory SO (17). Above all CsA is used (14, 56), which we ourselves have most often used to treat SO in the last decade. Recently the possibility of SO therapy using biological treatment by adalimumab has been discovered, with the aim of influencing cytokine mechanisms and TNF (tumour necrosis factor) (40), and also as supplementary therapy in the case of its refractory form (30). An addition to systemic therapy of SO is intravitreal application of aflibercept in order to remove the choroidal neovascular membrane (64), and dexamethasone to suppress cystoid edema (81). It still applies that the only prevention of SO of the second eye is timely enucleation of the irritated blind injured eyeball, but there is no uniform consensus on this (3, 13). Large studies present enucleations in the case of SO, in 100% (n = 105) (51) and in 28% (n = 130) (78) respectively. Czech and Slovak studies in summary present enucleation in 68% of cases. Following ocular injuries, evisceration of the eyeball is recommended before enucleation only in cases with a low risk of SO (3, 82), since there is a risk of insufficient removal of the uveal tissue remaining in the emisaries (3). Later enucleation following activation of SO has no influence on its course (14, 56).
Differential diagnosis of sympathetic ophthalmia. In our region it is necessary to consider above all phacoantigenic uveitis, which represents a set of pathologies with differing clinical symptoms, pathological mechanisms and histological verifications (18, 76). For this reason several types of uveitis generated by lens materials have been distinguished (54): phacotoxic non-granulomatous anterior uveitis, granulomatous uveitis triggered by lens materials, non-specific infiltration with macrophage reaction to lens materials, phacoanaphylactic endophthalmitis of non-infectious etiology. In the literature the term phacoanaphylactic uveitis is also used (12). The reason for this differential diagnostic view is the mechanism of origin (injury and postoperative state) and the similarity of the initial clinical stages of the pathology. In SO this predominantly concerns a T-lymphocyte reaction in all parts of the uveal tissue within the framework of remote cellular hypersensitivity, whereas in the case of phacoantigenic uveitis this concerns a reaction to a lens antigen within the framework of cytotoxic or immune complex hypersensitivity (18, 54) with the participation of an Arthus reaction of B-lymphocyte (12). Nevertheless, the most significant influence in the mechanism of phacoantigenic (phacoanaphylactic) uveitis is exerted by macrophages (18). The inflammatory granulomatous reaction is concentrated predominantly around damaged lens (16). Absolute differentiation of SO from phacoantigenic uveitis is enabled only by precise histological verification (in blind eyeballs), as was performed on our patients. Several times we recorded bilateral uveal irritation following unilateral injuries, which could correspond to cytotoxic or immune complex hypersensitivity.
Prognosis of sympathetic ophthalmia. SO is a very serious ocular pathology with a poor prognosis of vision, as a result of which timely diagnosis and sufficient therapy exerts a fundamental influence (14). Timely enucleation of the exciting and initiating eye has been considered necessary for a good prognosis of vision of the sympathising eye (51), which still applies for blind and long-term irritated eyes. Relapse of the pathology is very probable, despite the fact that many patients live without symptoms of this inflammation for many years (14). We ourselves recorded a relapse of SO which occurred after 38 years of a pacific condition. This contrasted with another patient, in whom there was permanent remission of the pathology at the end of the study for 32 years. Vision may be fundamentally influenced by complications: cataract, glaucoma and macular edema. In order to retain remission of SO it is necessary to ensure long-term immunosuppressant therapy (14). In all three patients with SO whom we are continuing to monitor up to now, we are continuing with a maintenance dose of immunosuppressants.
The first part of this study was supported by the project IGA 1152-3
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received: 5. 9. 2019
Accepted: 30. 10. 2019
Available on-line: 15. 2. 2020

MUDr. Jan Krásný
Oční klinika FNKV
Šrobárova 50
100 34 Praha 10
Sources
1. Ahmad N., Salvi S., Rudle PA. et al.: Sympahtetic ophthalmia after ruthenium plaque brachytherapy. Br J Ophtalmol, 91; 2007 : 399–401.
2. Al-Halafi A., Dhibi HA., Hamade IH. et al.: The association of systematic disorders with Vogt-Koyanagi-Harada and sympathetic ophthalmia. Graefes Arch Clin Exp Ophthalmol, 249; 2011 : 1229–1233.
3. Arevalo JF., Garcia RA., Al-Dhibi HA. et al.: Update on sympathetic ophthalmia Middle East Afr J. Ophthalmol, 19; 2012 : 13–21.
4. Aujla JS., Lee GA., Vincent, SJ. et al.: Incidence of hypotony and sympathetic ophthalmia following transscleral cyclophotocoagulation for glaucoma and a report of risk factors. Clin Experiment Ophthalmol, 41; 2013 : 761–772.
5. Auw-Haedrich C., Loeffler KU., Witschel H.: Sympathetic ophthalmia: an immunohistochemistry study of four cases. Ger J Ophthalmol, 5; 1996 : 98–103.
6. Aziz HA., Flynn HW., Young RC. et al.: Sympathetic ophthalmia: clinicopathologic correlation in a consecutive case series. Retina, 35, 2015 : 1696–1703.
7. Bartisch G.: ОFTALMOLOGIA (Augendienst). Stockel, Dressden, 1583, p. 205.
8. Brour J., Desjardins L., Lehoang P. et al.: Sympathetic ophthalmia after proton beam irradiation for choriodal melanoma. Ocul Immunol Inflamm, 20; 2012 : 273–6.
9. Brouzas D., Koutsandrea C., Moschos M. et al.: Massive choriodal hemorrhagae after intravitreal administration of bevacizumab (Avastin) for AMD followed by controlateral symphatetic ophthalmia. Clin Ophthalmol, 3; 2009 : 457–9.
10. Bruckner Z.: Ophtalmia sympathica in luetico po perforovaném plazivém vředu. Oftalmologický Sborník, 2; 1928 : 393 – 424.
11. Chan CC., Beneza D., Rodrigues MM. et al.: Immunohistochemistry and elektron microscopy of chorioidal infiltrates and Dalen-Fuchs nodules in sympathetic ophthalmia. Ophthalmology. 92; 1985 : 580–590.
12. Chan CC.: Relationships between sympathetic ophtalmia, phacoanaphylactic endophtalmitis and Vogt-Koyanagi-Harada disease. Ophthalmology, 95; l988 : 619 –624.
13. Chan CC., Roberge RG., Whitcup SP. et al.: 32 Case of sympathetic ophthalmia. A retrospective study at the National Eye Institute, Bethesda, Md., from 1982 to 1992. Arch Ophtalmol, 113; 1995 : 597–600.
14. Chan CC., Roberge FG.: Sympathetic Ophthalmia. In Pepose JS, Holland GJ, Wilhelmus KR.: Ocular Infection & Immunity, Mosby, New York, 1996, pp. 723–733. 15.Chang GC., Young LH.: Sympathetic ophtalmia. Semin Ophtalmol, 26; 2011 : 316–320.
16. Chen S., Aronow ME., Wang C. et al.: Classical pathology of sympathetic ophthalmia presented in a unique case. Open Ophthamol, 8; 2014 : 32–38.
17. Chu XK., Chan CC.: Sympathetic ophthalmia: to the twenty-first century and beyond. J Ophthalmol Inflamm Infect, 3; 2013 : 49–56.
18. Cousin CW., Kraus-Mackiw E.: Lens-associated uveitis. In Pepose JS, Holland GJ, Wilhelmus KR: Ocular Infection & Immunity, Mosby, New York, 1996, pp. 507–528.
19. Dienstbier E.: Konečná zpráva o výsledku léčby sympatické oftalmie penicilinem. Cs Oftal, 4; 1948 : 408–411.
20. Duke-Elder S (ed.): Text Book of Ophthalmology, Vol. IX. Disease of the uveal tract., Mosby, St.Louis, 1954, pp. 558–593.
21. Eckschlager T., Kasal P., Smetana K.: Některé možnosti využití nukleolárního testu v klinické diagnostice. Prakt Lek, 60; l980 : 667–68.
22. Elschnig A.: Die antigena Wirkung des Augenpigmentes. Albrecht von Graefes Arch Ophthalmol, 76; 1910 : 509.
23. Friedlaender MH.: Alergy and Immunology of the Eye, Raven Press, NewYork, 1993, pp. 206–212.
24. Fries PD., Char DH., Craford JB., et al.: Sympathetic ophthalmia complicating helium ion irradiation of a choriodal melanoma. Arch Ophthalmol, l05; l987 : 1561–64.
25. Fuchs E.: Über sympathisierende Entzündung zuerst bermerkungeen über seröse traumatische Iritis. Albrecht von Graefes Arch Ophthalmol, 61; 1905 : 365.
26. Fučíková T.: Imunologie. Vnitřní lékařství, Sv.V. Galén, Praha, 2002, 58 s.
27. Furusato E, Shen DF, Cao X, et al.: Inflammatory Cytokine and Chemokine Expression in Sympathetic Ophthalmia. Histol Histpatol, 26; 2011 : 1145 51.
28. Gass J.: Sympathetic ophthalmia after vitrectomy. Am J Ophthal, 93; l982 : 552–58.
29. Garcia-Arumi J., Montolio GM., Morral M. et al.: Sympathetic ophthalmia after surgical resection of iridociliary melanoma. Graefes Arch Clin Exp Ophthalmol, 244; 2006 : 1353–1356.
30. Hiyama T., Harada Y., Kiuchi Y.: Effective treatment of refractory sympathetic ophthalmia with glaucoma using adalimumab. Am J Ophthalmol Case Rep, 14; 2019 : 1–4.
31. Hrabánek J., Lukášová M., Smetana K.: Monitorování aktivních lymfocytů v periferní krvi pacientů po transplantaci kostní dřeně. Cas Lek Ces, 133; 1994 : 80–2.
32. Ibragimova NV., Tugolukova LV., Kravtsov V. et al.: The number of nucleoli in peripheral blood lymphocytes of the Chernobyl accident liquidator. Tsitologia, 43; 2001 : 941 43.
33. Inouye S., Ideta H., Ishikova H., et al.: Sympathetic ophthalmia following vitrectomy and /or retinal detachment surgery. Acta Soc Ophthalmol, 92; l988 : 372–376.
34. Jakobiec FA., Lefkowitch J., Knowles II. DM.: B - and T-lymphocytes in ocular diseases. Ophthalmology, 91; 1984 : 635 654.
35. John J., Iserle J.: Korepraxe fotokoagulací a sympatická oftalmie. Cesk Slov Oftalmol, 33; 1977 : 377–82.
36. Kaneko Y., Wu GS., Saraswathy S. et al.: Immunopathologic processes in sympathetic ophthalmia as signified by microRNA profiling. Invest Ophthalmol Vis, Sci, 53; 2012 : 4197–204.
37. Kaplan H., Waldrep JC., Chan WC. et al.: Human sympathetic ophthalmia immunologic analysis of the vitreous et uvea. Arch Ophthalmol, 104; l986 : 240–4.
38 Karel I., Krejčí L.: Naše dosavadní zkušenosti při léčbě sympatické oftalmie. Cesk Slov Oftalmol, 14; 1958 : 468–471.
39. Kavka J.: K prevenci a léčbě soucitného onemocnění. Cesk Slov Oftalmol, 23; 1967 : 212–4.
40. Kim JB., Jeroudi A., Angels-Han ST. et al.: Adalimumab for pediatric sympathetic ophthalmia. JAMA Ophthalmol, 132; 2014 : 1022–24.
41. Kilmartin DJ., Dick AD., Forrester JV.: Prospective surveillance of sympathetic ophthalmia in the UK and republic of Ireland. Brit J Ophthalmol, 84; 2000 : 259–263.
42. Klimartin DJ., Wilson D., Liversidge J. et al.: Immunogenetics and clinical phenotype of sympathetic ophthalmia in British and Irish patients. Br J Ophthalmol, 85; 2001 : 281–286.
43. Korčáková L., Reneltová J., Hašková V.: Možnost diagnostiky při transplantaci ledvin podle morfologie nukleolů cirkulujících lymfocytů, Cas Lek Ces, 114; 1975 : 616–618.
44. Korčáková L., Pekárek J., Rovenský J. et al.: Lymphocyte nucleolar activation as a marker of autoimmune disorders. Immunology 31; 1976 : 803–805.
45. Krásná J., Mezerová V., Krásný J.: Hodnocení efektivnosti léčby neinfekčních uveitid. Cesk Slov Oftalmol, 69; 2013 : 110–116.
46. Krásný J.: Závěrečná zpráva IGA 1152-3: Komplexní hodnocení péče o děti s imunopatologickým onemocněním oka, 1992–1994.
47. Krásný J.: Uvea. In Kolín J, a kol.: Oftalmologie praktického lékaře. Karolinum, Praha, 1994, s. 9–111.
48. Krásný J., Honzová S.: Vogt-Koyanagi-Harada syndrom u dětí. Cesk Slov Oftalmol, 51; 1995 : 156–165.
49. Kyoichi O., Shinji K., Keiji O. et al.: Surface markers of periferal blood lymphocytes in Vogt-Koyanagi-Harada diseases. J Clin Lab Immunol, 17, 1985 : 49–52.
50. Lam S., Tessler HH., Lam BL. et al.: High incidence of sympathetic ophthalmia after contakt and noncontact neodymiumYAG-cyclotherapy. Ophthalmology, 99; l992 : 1818–2.
51. Lubin JR., Albert DM., Weinstein M.: Sixty-five years of sympathetic ophthalmia. A clinicopathologic review of 105 cases 1913-1978. Ophthalmology, 87; l980 : 109–121.
52. MacKenzie W.: A practical treatment on the diseases of the eye. 3rd ed. Longman, London, 1840: pp. 523–534.
53. Muakkassa NW., Witkin AJ.: Spectral-domain optical coherence tomography of sympathetic ophthalmia with Dalen-Fuchs nodules. Ophthal Surg Lasers Imaging Retina. 45; 2014 : 610–612.
54. Müller-Hermelink HK., Kraus W.: Recent topic in the pathology of uveitis. In Kraus-Mackiw E, O´Connor GR: Uveitis, Pathophysiology and Therapy, Thieme-Stratton Inc., New York, l986, pp. 155–203.
55. Nguyen AM., Rao NA.: Oxidative photoreceptor cell damage in autoimmune uveitis. J Ophthalmol Inflamm Infect, 1; 2011 : 7–13.
56. Nussenblatt RB., Palestine AG.: Uveitis, Fundamentals and Clinical Practice, YBMP, New York, l989, pp. 257 273.
57. Oláh Z.: Príspevok k patologii sympatickej oftalmie. Cesk Slov Oftalmol, 23; 1967 : 35–40.
58. Parvaresh MM., Falavarjani KG.: Presumed sympathetic ophthalmia after scleral bucking surgery. Retin Cases Brief Rep, 4; 2013 : 331–333.
59. Patel SS., Dodds EM., Echandi LV. et al.: Long-term, drug-free remission of sympathetic ophthalmia with high-dose, short-term chlorambucil therapy. Ophthalmology, 121; 2014 : 596–602.
60. Pusey B.: Cytotoxin and sympathetic ophthalmia. Arch Ophthalmol, 32; 1903: p. 334.
61. Rao NA.: Mechanisms of imflammatory response in sympathetic ophthalmia and VKH syndrome. Eye, 11; 1997 : 213–216.
62. Reynard M., Shulman IA., Azen, SP. et al.: Histocompatibility antigens in sympathetic ophthalmia. Am J Ophthalmol, 95; l983 : 216–221.
63. Roberts F., Chee KT.: Lee´s Ophtalmic Histopathology, 3th ed., Springer-Verlang, London, 2014, 466 pp.
64. Saatci AO., Ayhan Z., Ipek SC. et al.: Intravitreal Aflibercept as an adjunct to systemic therapy in a case chorioidel neovascular membrane associated with sympathetic ophthalmia. Turk J Ophthalmol, 48; 2018 : 208–11.
65. Shen J., Fang W., Jin XH. et al.: Sympathetic ophthalmia caused by a severe ocular chemical burn: a case report and literature review. Int J Clin Exp Med, 8; 2015 : 2974–8.
66. Sisk RA., Davis JL., Dubovy SROV., et al.: Symphatetic ophthalmia following vitrectomy for endophtalmitis after intravitreal bevacizumab. Ocul Immunol Inflamm, 16; 2008 : 236–238.
67. Smetana K.: Poznámky k vyšetřovaní nukleolů v lymfocytech. Imunol Zpravodaj, 7; l976 : 399–419.
68. Smetana K.: A futher contribution on the question of the incidence of nucleoli in the nuclei of mature lymphocytes in man. Folia Biol (Praha), 7; 1961 : 268–274.
69. Smetana K., Freireich, EJ., Busch H.: Chromatin structures in ring-shaped nucleoli of human lymphocytes. Exptl Cell Res, 52; 1968 : 112-128.
70. Smetana K., Gyorkey F., Gyorkey P. et al.: Comparative studies on the ultrastructure of nucleoli in human lymphosarcoma cells and leukemic lymphocytes. Cancer Research, 30; 1970 : 1149–55.
71. Smetana K., Lejnar J., Potměšil M.: A futher contribution to the demonstration of RNA and nucleoli of blood cells in smear preparations. Folia Haemat, 91; 1969 : 4–9.
72. Smetana K., Lejnar J., Sálková J.: Studies on nucleoli in rossetting T and B lymphocytes of the human peripheral blood. Folia Haematol Int Klin Morphol Blutforsch, 107; 1980 : 720–7.
73. Smetana K., Rosa L., Šubrtová H. et al.: Futher studies on satellite nucleoli of lymphocytes in patients suffering from B chronic lymphatic leukaemia. Int J Tissue React, 16; 1994 : 181–185.
74. Sváčová H., Izák M., Timová S. et al.: Sympatická oftalmia. Cesk Slov Oftalmol, 40, 1990 : 218–222.
75. Svozílková P., Říhová .E, Brichová M. et al.: Sympatická oftalmie. Cesk Slov Oftalmol, 62; 2006 : 218–223.
76. Svozílková P.: Sympatická oftalmie. In Říhová E, a kol.. Uveitidy, Praha, Grada, 2009, s. 59–60.
77. Štepán J., Smetana K., Smolíková M. et al.: Lymphocyte nucleoli in the peripheral blood and knee joint effusions in patients with rheumatoid arthritis. Z Rheumatol, 37; 1978 : 40–4.
78. Tan XL., Seen S., Dutta-Majumder P. et al.: Anylysis of 130 cases of sympathetic ophthalmia – a retrospective multicenter case series. Ocul Imunol Inflamm, 12; 2018 : 1–8.
79. Toriyama K., Miyajima Y., Lijima F.: Two cases of sympathetic ophthalmia following in intraocular lens Implantation Folia Ophthalmol, 40; l989 : 32–5.
80. Tyagi M., Agarwal K., Reddy Pappuru RR. et al.: Sympathetic ophthalmia after vitreoretinal surgeries: incidence, clinical presentations and outcomes of rare disease. Semin Ophthalmol, 32; 2019 : 157–62.
81. Vejdovský V.: Sympathická ophtalmie po operaci šedého zákalu. Oftalmologický Sborník, 7; 1932 : 109 – 111.
82. Wocker L., Januschowski K.: Steroid implant in treatment of sympathetic ophthalmia: intravitreal implant of dexamethasone in cystoid macular edema in the context of sympathetic ophthalmia. Ophthalmologe, 116; 2019 : 380–3.
83. Zheng C., Wu AY.: Enucleation versus evisceration in ocular trauma: a retrospective review and study of current literature. Orbit, 32; 2013 : 356–61.
Labels
OphthalmologyArticle was published in
Czech and Slovak Ophthalmology

2019 Issue 5
Most read in this issue
- Molecular genetic cause of achromatopsia in two patients of Czech origin
- INTRAVITREAL THERAPY OF ENDOGENOUS ENDOPHTALMITIS DUE TO UROSEPSIS – A CASE REPORT
- Sensitivity and specificity of spectral OCT in patients with early glaucoma.
- The long-term monitoring of sympathetic ophthalmia in the diagnostic and terapeutic view. Review Department of Ophthalmology