
Intestinal pseudo-obstruction syndrome in a patient with acute polyradiculoneuritis
Authors:
K. Šimková 1; L. Ungermann 2; E. Ehler 1,3; I. Štětkářová 4
Authors‘ workplace:
Department of Neurology Pardubice Regional Hospital, Czech Republic
1; Radiodiagnostic Department of the Pardubice Regional Hospital, Czech Republic
2; Department of Neurology, Faculty of Health Studies, University of Pardubice, Czech Republic
3; Department of Neurology, Third Faculty of Medicine, Královské Vinohrady University Hospital, Prague, Czech Republic
4
Published in:
Cesk Slov Neurol N 2026; 89(3): 199-201
Category:
Letter to Editor
doi:
https://doi.org/10.48095/cccsnn2026199
Dear Editor,
Acute colonic pseudo-obstruction (ACPO) is characterized by acute colonic dilatation in the absence of a mechanical obstruction. It occurs in a variety of settings, including inflammatory, neoplastic, post-traumatic, and systemic conditions. Progressive colonic distension may lead to ischaemia and subsequent perforation in approximately 15% of patients, with an associated mortality rate of up to 40% [1]. In 1948, Sir William Ogilvie described two patients with pseudo-obstruction syndrome associated with malignant infiltration of the prevertebral ganglia [2].
Autonomic innervation of the intestinal wall and its imbalance play a crucial role in the pathophysiology of intestinal pseudo-obstruction. Ogilvie originally attributed this condition to deprivation of sympathetic innervation [2]. However, current evidence suggests a predominance of sympathetic tone with reduced parasympathetic activity. Impaired parasympathetic innervation, particularly in the distal colon, results in an atonic segment and functional obstruction [3].
Among the wide range of conditions associated with intestinal pseudo-obstruction, neurological disorders such as Parkinson’s disease, other neurodegenerative diseases, and drug-induced states (e. g., due to sedatives) are commonly reported [4]. Polyneuropathies are rarely implicated, and only a limited number of reports describe an association with Guillain–Barré syndrome [5]. We present a case of a 78-year-old patient with acute inflammatory demyelinating polyradiculoneuritis (AIDP) complicated by severe intestinal pseudo-obstruction.
A 78-year-old man was admitted to the Department of Neurology on November 18, 2024 with acute onset of upper and lower limbs weakness and paraesthesias of the hands and feet, which began earlier that morning. During the day, both motor weakness and sensory disturbances progressed, predominantly in the distal extremities (tactile hypesthesia). At approximately 17 : 30, while attempting to walk to the toilet with forearm crutches, his legs gave way and he was unable to stand.
Neurological examination revealed moderate quadriparesis, more pronounced distally. The patient was able to hold his head elevated for up to 20 s. Grip strength measured 26 kPa in the right hand and 22 kPa in the left. In the outstretched arm position, the right arm dropped within 4 s, whereas the left was maintained for more than 20 s. Lower limb elevation was sustained for 15 s on the right and 20 s on the left. Cranial nerves were intact. Sensory examination showed impairment (tactile hypesthesia) in the distal halves of the hands and fingers and approximately 10 cm below the patella bilaterally; vibration sense was absent in the lower limbs.
Electromyography performed on November 21 confirmed a demyelinating polyradiculoneuropathy. Cerebrospinal fluid analysis demonstrated protein-cytological dissociation (protein 0.64 g/L, leukocyte count 1/μL), confirming the diagnosis of AIDP. Intravenous immunoglobulin therapy (Kiovig, total dose 2 g/kg over 5 days) was administered, resulting in mild clinical improvement. Brain CT (November 18 2024) was unremarkable; brain MRI (November 20) revealed multiple small non-expansive lesions and an arachnoid cyst in the left temporal region.
The patient was a retired clerk. His medical history included trial fibrillation (since 2009) treated with repeated cardioversions (CHA₂DS₂-VASc score 2) and long-term anticoagulation with dabigatran. Following amiodarone therapy, he had maintained sinus rhythm since 2022. Additional comorbidities included arterial hypertension, impaired glucose tolerance, dilation of the ascending aorta, and renal cysts. He had a history of COVID-19 infection in December 2021.
The clinical course became complicated on November 26, when the patient developed abdominal pain, hypogastric tenderness, and mild enterorrhagia, accompanied by mild anaemia. Abdominal ultrasound revealed meteorism and a right renal cyst. On November 29, his condition deteriorated, with subfebrile temperature, lethargy, leukocytosis (18,6), and potassium levels ranging from 3.5–4.4 mmol/L. Chest X-ray showed no signs of pneumonia but revealed elevation of the right hemidiaphragm. Oral intubation and mechanical ventilation installed.
On December 2, the patient developed diffuse abdominal pain, recurrent vomiting, abdominal distension with tympanic percussion, and reduced bowel sounds. Urgent abdominal CT demonstrated massive dilatation of the caecum and ascending colon (115 × 125 mm), elevation of the right hemidiaphragm, and compressive atelectasis of the middle and lower lobes (Fig. 1). Based on clinical and radiological findings, a diagnosis of ACPO (Ogilvie syndrome) was established. Conservative management was initiated, including neostigmine (0.5 mg s.c. every 6 h), rectal decompression, dietary restriction, and consideration of endoscopic decompression; however, endoscopic intervention was not indicated.

C – slepé střevo; D – colon descendens; R – rektum; S – colon sigmoideum
Despite initial stabilization, the patient’s condition worsened again on 10 December, with hypoxaemia, dyspnoea, deteriorating respiratory function, and signs of incipient sepsis. Chest imaging confirmed right-sided pneumonia. The patient was transferred to the neurological intensive care unit, intubated, and placed on mechanical ventilation with vasopressor support and analgosedation. Bronchoscopy with airway toileting was performed, and antibiotic therapy with cefotaxime was initiated.
By December 16, inflammatory markers had decreased, although severe flaccid quadriparesis persisted. A tracheostomy was performed. Gradual clinical improvement followed, with resolution of abdominal distension under prokinetic therapy and partial regression of pulmonary findings. The patient was transferred to the Department of Anaesthesiology and Resuscitation.
By December 18, the patient was conscious, cooperative, and communicative. Abdominal findings had significantly improved. Antibiotic therapy was discontinued on December 26. Mechanical ventilation was terminated on January 1, 2025, and intensive rehabilitation was initiated. On January 30, the patient was transferred to a rehabilitation facility. At that time, he was off prokinetic therapy, tolerating a puréed diet, able to sit independently, and ambulate with a walker. Gastrointestinal function was stable.
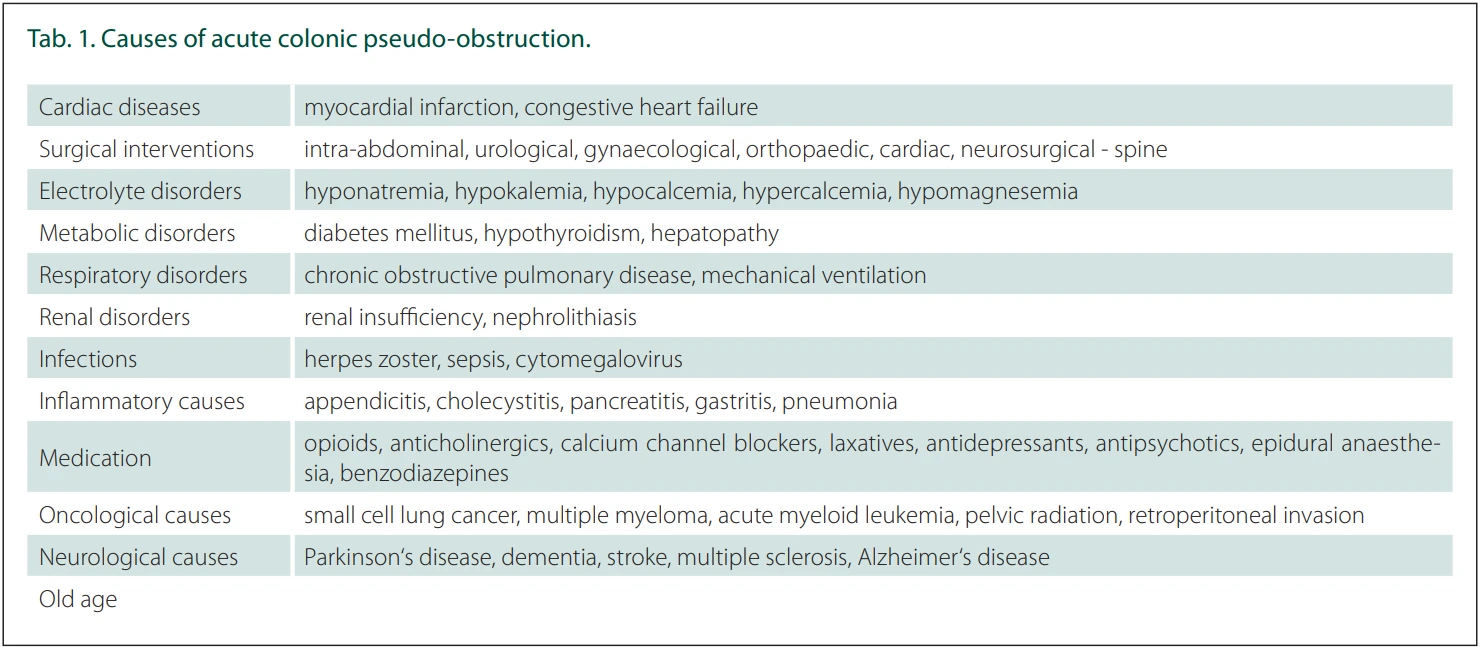
Neurological causes account for approximately 27% of ACPO cases and include stroke, Parkinson’s disease, medications (e. g., antidepressants, antipsychotics, antiparkinsonian drugs), and electrolyte disturbances such as hypokalaemia [6]. Colonic motility depends heavily on autonomic innervation, with peristaltic activity typically originating in the caecum and propagating distally (Tab. 1). The transition zone is located near the splenic flexure, reflecting the interface between vagal and sacral parasympathetic innervation. Dysfunction of this autonomic regulation, involving the enteric nervous system and interstitial cells of Cajal, results in impaired motility [2].
Both reduced and uncoordinated autonomic stimulation may lead to severe motility disturbances. Although Guillain–Barré syndrome associated with intestinal pseudo-obstruction has been reported, it remains rare [5]. Our findings are consistent with previously published cases [7–10].
ACPO must be distinguished from paralytic ileus and mechanical obstruction. While ileus may result from vascular compromise or mechanical causes, pseudo-obstruction presents with marked colonic dilatation without an identifiable obstruction, potentially progressing to ischaemia and perforation.
The incidence of ACPO has decreased in recent years. Wells et al. (2017) reported approximately 100 cases per 100,000 hospital admissions, with mortality reduced to 6.4% from previously reported rates of up to 30% [2]. However, complications such as perforation or ischaemia still occur in 10–20% of cases and are associated with high mortality.
Diagnosis is primarily based on imaging findings. Caecal dilatation exceeding 12 cm is associated with a high risk of ischaemia and perforation [1]. In our case, significant dilatation was observed without progression to perforation.
Management of ACPO is primarily conservative. Neostigmine is effective and typically produces a rapid response within 5–30 minutes. Additional prokinetic agents include metoclopramide, erythromycin, and cisapride. Prucalopride, a selective 5-HT4 receptor agonist, represents a newer therapeutic option. Endoscopic or surgical interventions are reserved for refractory cases or complications. Recurrence rates range from 18% to 33%.
We report a rare case of AIDP complicated by severe ACPO. Early recognition and multidisciplinary management were essential for a favourable outcome. The patient survived a life-threatening condition and continues rehabilitation with gradual functional improvement.
Fig. 2. The entire abdomen is displayed in the supine position on the so-called “toposcan”, which is used for planning CT scans. There is a superficial dilatation of the colon by gas with a maximum in the caecum and colon sigmoideum.
Obr. 2. Celá břišní dutina je zobrazena v poloze na zádech na tzv. „toposcanu“, který se používá k plánování CT vyšetření. Je patrná povrchová dilatace tlustého střeva způsobená plynem, s maximem v slepém střevě a sigmatu.

Fig. 3. Postcontrast CT scan with a reconstruction of 3mm layers in the sagittal plane. Dilatation of the colon sigmoideum (S – colon sigmoideum, R – rectum).
Obr. 3. CT vyšetření po podání kontrastní látky s rekonstrukcí v 3mm vrstvách v sagitální rovině. Dilatace sigmatu (S – sigmoid, R – konečník).

Conflict of interest
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
Sources
1. Underhill J, Munding E, Hayden D. Acute colonic pseudo-obstruction and volvulus: pathophysiology, evaluation, and treatment. Clin Colon Rectal Surg 2021; 34 (4): 242–250. doi: 10.1055/s-0041-1727195.
2. Wells CI, O‘Grady G, Bissett IP. Acute colonic pseudo-obstruction: a systematic review of aetiology and mechanisms. World J Gastroenterol 2017; 23 (30): 5634–5644. doi: 10.3748/wjg.v23.i30.5634.
3. Arthur T, Burgess A. Acute colonic pseudo-obstruction. Clin Colon Rectal Surg 2022; 35 (3): 221–226. doi: 10.1055/s-0041-1740044.
4. Vanek P, Urban O, Falt P. Percutaneous endoscopic cecostomy for management of Ogilvie’s syndrome: a case series and literature Review with an update on current guideline. [online]. Available from: https: //doi.org/10.1007/s00464-023-10281-w.
5. Pérez-Lara JL, Santana Y, Hernández-Torres J et al. Acute colonic pseudo-obstruction caused by dexmedetomidine: a case report and literature review. Am J Case Rep 2019; 20 : 278–284. doi: 10.12659/AJCR.913645.
6. Haj M, Haj M, Rockey DC. Ogilvie‘s syndrome: management and outcomes. Medicine (Baltimore) 2018; 97 (27): e11187. doi: 10.1097/MD.0000000000011187.
7. Man BL, Fu YP. Intestinal pseudo-obstruction as a presenting symptom of Guillain-Barré syndrome. BMJ Case Rep 2014; 2014: bcr2014205155. doi: 10.1136/bcr-2014-205155.
8. Ramirez R, Zuckerman MJ, Hejazi RA et al. Treatment of acute colonic pseudo-obstruction with tegaserod. Am J Med Sci 2010; 339 (6): 575–576. doi: 10.1097/MAJ.0b013e3181db6b95.
9. Sahu TA. An atypical descending variant of guillain-barré syndrome with bulbar palsy, autonomic instability, and delayed colonic pseudo-obstruction: a case report. Cureus 2025; 17 (10): e95802. doi: 10.7759/cureus.95802.
10. Luo L, Chen L, Li J et al. Case report: successful treatment of severe Guillain-Barré syndrome with paralytic ileus as a presenting symptom by intensive immunotherapy. Front Immunol 2025; 16 : 1435817. doi: 10.3389/fimmu.2025.1435817.
11. Diagnosis is primarily based on imaging findings. Caecal dilatation exceeding 12 cm is associated with a high risk of ischaemia and perforation [1]. In our case, significant dilatation was observed without progression to perforation.
12. Management of ACPO is primarily conservative. Neostigmine is effective and typically produces a rapid response within 5–30 minutes. Additional prokinetic agents include metoclopramide, erythromycin, and cisapride. Prucalopride, a selective 5-HT4 receptor agonist, represents a newer therapeutic option. Endoscopic or surgical interventions are reserved for refractory cases or complications. Recurrence rates range from 18% to 33%.
Labels
Paediatric neurology Neurosurgery NeurologyArticle was published in
Czech and Slovak Neurology and Neurosurgery

2026 Issue 3
Most read in this issue
- 100 years of the Czech Department of Neurology, Charles UniversityThe Henner school
- Intestinal pseudo-obstruction syndrome in a patient with acute polyradiculoneuritis
- Perinatal ischemic stroke – a review of current knowledge
- Epilepsy surgery in children operated on before 3 years of age – experience of the Motol epilepsy center